Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Ayesha Sadiqa 2015-Phd-Chemistry-03 Supervisor Prof. Dr. Syeda Rubina Gilani Department of Chemistry University of Engineering and Technology, LahoreDokument21 SeitenAyesha Sadiqa 2015-Phd-Chemistry-03 Supervisor Prof. Dr. Syeda Rubina Gilani Department of Chemistry University of Engineering and Technology, LahoreRahi FurqanNoch keine Bewertungen
- Pentavalent VaccineDokument1 SeitePentavalent VaccineMani Seshan100% (1)
- Types of Culture MediaDokument7 SeitenTypes of Culture MediaSurbhi GuptaNoch keine Bewertungen
- Microbiology Work InstructionsDokument58 SeitenMicrobiology Work InstructionsJam SanchezNoch keine Bewertungen
- MicroparaDokument4 SeitenMicroparanormanyasis319512Noch keine Bewertungen
- Week 1:: A Case For Evolutionary Thinking: Understanding HIV 1Dokument14 SeitenWeek 1:: A Case For Evolutionary Thinking: Understanding HIV 1JeevikaGoyalNoch keine Bewertungen
- An Overview of Inclusion Body Hepatitis-Hydropericardium Syndrome (IBH-HPS)Dokument26 SeitenAn Overview of Inclusion Body Hepatitis-Hydropericardium Syndrome (IBH-HPS)kedar karkiNoch keine Bewertungen
- 'Docslide - Net - West Nile FeverDokument23 Seiten'Docslide - Net - West Nile Feverirsyad120Noch keine Bewertungen
- SA Health Cleaning Standard 2014 - (v1.1) CDCB Ics 20180301 PDFDokument48 SeitenSA Health Cleaning Standard 2014 - (v1.1) CDCB Ics 20180301 PDFPham PhongNoch keine Bewertungen
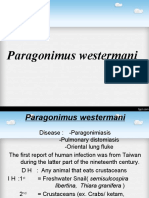
- Kuliah Paragonimus WestermaniDokument17 SeitenKuliah Paragonimus WestermaniIda Bagus Putu SwabawaNoch keine Bewertungen
- Microbial Flora of Human BodyDokument2 SeitenMicrobial Flora of Human BodyIah Kriztel BagacinaNoch keine Bewertungen
- En Oie Asf Poc Tests Guide FinalDokument13 SeitenEn Oie Asf Poc Tests Guide Finaljefry ManurungNoch keine Bewertungen
- Klasifikasi VirusDokument3 SeitenKlasifikasi VirusADINoch keine Bewertungen
- Latihan SN f5 Tahun Baru CinaDokument4 SeitenLatihan SN f5 Tahun Baru CinaMohd Rizal RazakNoch keine Bewertungen
- MLT 107 Chapter 3 5 Infection Cont and QADokument29 SeitenMLT 107 Chapter 3 5 Infection Cont and QACristina CunhaNoch keine Bewertungen
- Thrive The GameDokument2 SeitenThrive The GameNational Catholic ReporterNoch keine Bewertungen
- Leture 3Dokument70 SeitenLeture 3Ziqian HENoch keine Bewertungen
- BacteriophageDokument311 SeitenBacteriophageThị Sô Phia100% (1)
- Rosen's Emergency Medicine Concepts and Clinical PracticeDokument15 SeitenRosen's Emergency Medicine Concepts and Clinical PracticeMusdal RahmatNoch keine Bewertungen
- Solanum Lycopersicum Bacillus Subtilis: TITLE: Analysis of The Antimicrobial Activity of Lycopene (CDokument3 SeitenSolanum Lycopersicum Bacillus Subtilis: TITLE: Analysis of The Antimicrobial Activity of Lycopene (CKristal Jade de LiraNoch keine Bewertungen
- Ghannoum, Mahmoud A. - Perfect, John R - Antifungal therapy-CRC Press (2019)Dokument537 SeitenGhannoum, Mahmoud A. - Perfect, John R - Antifungal therapy-CRC Press (2019)Defne Güller100% (1)
- Blood Stream Infections With Candida Species: A Prospective Study in A Tertiary Care CenterDokument7 SeitenBlood Stream Infections With Candida Species: A Prospective Study in A Tertiary Care CenterAkula Sai PrasannaNoch keine Bewertungen
- APVS 2005 Proceedings More On PigsDokument258 SeitenAPVS 2005 Proceedings More On PigsDulce AmorNoch keine Bewertungen
- FungiDokument2 SeitenFungiRia AlcantaraNoch keine Bewertungen
- Group2 Diagnostic Laboratory TestDokument16 SeitenGroup2 Diagnostic Laboratory TestKristle Anne Federigan - LacanlaleNoch keine Bewertungen
- Dengue IGG IGM X 10 All TestDokument1 SeiteDengue IGG IGM X 10 All TestKaren Ramos CardenasNoch keine Bewertungen
- HECP Paper With ANS KeyDokument6 SeitenHECP Paper With ANS KeyMyPharmapediaNoch keine Bewertungen
- Communicable Disease ActivitiesDokument11 SeitenCommunicable Disease ActivitiesPlacida Mequiabas National High SchoolNoch keine Bewertungen
- Lecture 14-15Dokument34 SeitenLecture 14-15Haswanth KolluNoch keine Bewertungen
- Poxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Dokument10 SeitenPoxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Mestesanu ElisabetaNoch keine Bewertungen