Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- CDC - Ventilator-Associated Pneumonia (VAP) EventDokument13 SeitenCDC - Ventilator-Associated Pneumonia (VAP) EventAl MuzakkiNoch keine Bewertungen
- NCP-Bronchial Asthma Without EvalDokument2 SeitenNCP-Bronchial Asthma Without EvalTrisha Lapid MatulaNoch keine Bewertungen
- 145 One Lung VentilationDokument6 Seiten145 One Lung VentilationEyad AbdeljawadNoch keine Bewertungen
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDokument5 SeitenPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNoch keine Bewertungen
- Hui Lin Lam - LinkedInDokument6 SeitenHui Lin Lam - LinkedInJack ChenNoch keine Bewertungen
- 10 MAX FUNDAMENTALES DE VM Chatburn - A Taxonomy of Mechanical Ventilation 2014 (With Supplemental)Dokument41 Seiten10 MAX FUNDAMENTALES DE VM Chatburn - A Taxonomy of Mechanical Ventilation 2014 (With Supplemental)evangemcpNoch keine Bewertungen
- Curvas y Bucles 5Dokument12 SeitenCurvas y Bucles 5Patty MArivel ReinosoNoch keine Bewertungen
- Asthma: History and Physical Findings: Ixsy Ramirez, MD, MPH Pediatric PulmonologyDokument32 SeitenAsthma: History and Physical Findings: Ixsy Ramirez, MD, MPH Pediatric Pulmonologyfurr singhNoch keine Bewertungen
- Therapist Driven ProtocolsDokument3 SeitenTherapist Driven ProtocolsPaoly PalmaNoch keine Bewertungen
- Guidelines For Pulmonary Rehabilitation Programs,.26Dokument1 SeiteGuidelines For Pulmonary Rehabilitation Programs,.26Amr Mohamed GalalNoch keine Bewertungen
- Asthma Lesson PlanDokument29 SeitenAsthma Lesson PlanRabiu Hassan Musa86% (7)
- Drugs Acting On The Respiratory SystemDokument13 SeitenDrugs Acting On The Respiratory SystemAlloiBialbaNoch keine Bewertungen
- Hypernatremia Hyperkalemia: of Increased Serum K+Dokument3 SeitenHypernatremia Hyperkalemia: of Increased Serum K+edited_chenNoch keine Bewertungen
- Jurnal Efusi PleuraDokument11 SeitenJurnal Efusi PleuraAri StefanusNoch keine Bewertungen
- The Mechanical VentilatorDokument28 SeitenThe Mechanical VentilatorJohn AlcantaraNoch keine Bewertungen
- Bronchial AsthmaDokument46 SeitenBronchial AsthmaKhor Kee GuanNoch keine Bewertungen
- PBL BurnDokument20 SeitenPBL Burn徐浩恩Noch keine Bewertungen
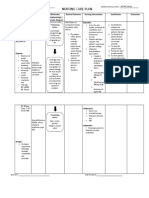
- Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDokument5 SeitenNursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale Evaluationkrish_tartNoch keine Bewertungen
- Ventilación Mecánica en Pacientes NeurocriticosDokument14 SeitenVentilación Mecánica en Pacientes NeurocriticosJoseph Campos SanchezNoch keine Bewertungen
- Foreign Bodies of Air Passages and Food PassageDokument20 SeitenForeign Bodies of Air Passages and Food PassageRamli HassanNoch keine Bewertungen
- Role of Physiotherapy in ICUDokument68 SeitenRole of Physiotherapy in ICUprasanna3k100% (2)
- RCT of Aprv Vs LPV in Ards PtsDokument11 SeitenRCT of Aprv Vs LPV in Ards PtsOldriana Prawiro HapsariNoch keine Bewertungen
- NCP To NG PneumoniaDokument3 SeitenNCP To NG PneumoniaGlenn Asuncion PagaduanNoch keine Bewertungen
- Corrected PFT JayatiDokument43 SeitenCorrected PFT JayatiKRIPAL BARDHANNoch keine Bewertungen
- Journal Homepage: - : Manuscript HistoryDokument5 SeitenJournal Homepage: - : Manuscript HistoryIJAR JOURNALNoch keine Bewertungen
- Chest and LungsDokument49 SeitenChest and LungsChala KeneNoch keine Bewertungen
- Spesifikasi - VYGON Emergency APO CPAP KitDokument2 SeitenSpesifikasi - VYGON Emergency APO CPAP KitNanno LadowogoNoch keine Bewertungen
- Pulmonary Function TestDokument19 SeitenPulmonary Function TestAshenafi BerhanuNoch keine Bewertungen
- COPDDokument2 SeitenCOPDejarnmdNoch keine Bewertungen