Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Wound Care PDFDokument100 SeitenWound Care PDFVanessaMUeller100% (2)
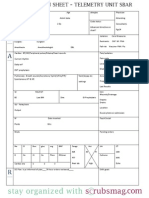
- Nurse Brain Sheet Telemetry Unit SBARDokument1 SeiteNurse Brain Sheet Telemetry Unit SBARvsosa624Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Nurse Brain Sheet With Shift HoursDokument2 SeitenNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- WB CC Critical Care Front MatterDokument18 SeitenWB CC Critical Care Front MatterkushishaNoch keine Bewertungen
- Feeding and Eating Disorders GuideDokument42 SeitenFeeding and Eating Disorders GuideCharlaine BacasnoNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Nurse Brain Sheet Half SizeDokument1 SeiteNurse Brain Sheet Half Sizevsosa624Noch keine Bewertungen
- Lab Values Chart GuideDokument5 SeitenLab Values Chart GuideVanessaMUeller100% (3)
- Alcohol Withdrawal Care PlanDokument1 SeiteAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- Newborn Assessment NORMALDokument2 SeitenNewborn Assessment NORMALVanessaMUellerNoch keine Bewertungen
- Nursing Management of A Patient With Close FractureDokument15 SeitenNursing Management of A Patient With Close FractureJoshuaYapNoch keine Bewertungen
- COPD Care PLAN PDFDokument2 SeitenCOPD Care PLAN PDFVanessaMUeller100% (1)
- Advia 2120i Hematology SystemDokument8 SeitenAdvia 2120i Hematology SystemDwitaRiadiniNoch keine Bewertungen
- ECG Procedural Cheklist With RationaleDokument3 SeitenECG Procedural Cheklist With RationaleCzarina Rachel RamirezNoch keine Bewertungen
- Hemolytic UremicsyndromeDokument60 SeitenHemolytic UremicsyndromeMuhammad AleemNoch keine Bewertungen
- Comprehensive Head To Toe Assessment PDFDokument22 SeitenComprehensive Head To Toe Assessment PDFVanessaMUellerNoch keine Bewertungen
- Endotracheal TubeDokument23 SeitenEndotracheal Tubeanayunita100% (1)
- Alcohol Withdrawal Care PlanDokument1 SeiteAlcohol Withdrawal Care PlanVanessaMUellerNoch keine Bewertungen
- Physical Assessment ChartDokument1 SeitePhysical Assessment ChartVanessaMUellerNoch keine Bewertungen
- Example 1 - Focus: Nausea Related To AnestheticDokument1 SeiteExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerNoch keine Bewertungen
- ManagmentDokument1 SeiteManagmentVanessaMUellerNoch keine Bewertungen
- Name Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXDokument1 SeiteName Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXVanessaMUellerNoch keine Bewertungen
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDokument1 SeiteFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerNoch keine Bewertungen
- Penuemonia Care PalnDokument2 SeitenPenuemonia Care PalnVanessaMUellerNoch keine Bewertungen
- Updated Clinical SheetDokument1 SeiteUpdated Clinical SheetVanessaMUellerNoch keine Bewertungen
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDokument1 SeiteFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerNoch keine Bewertungen
- Admission Database PDFDokument6 SeitenAdmission Database PDFVanessaMUellerNoch keine Bewertungen
- Diseases With Dermatologic ManifestationsDokument1 SeiteDiseases With Dermatologic ManifestationsVanessaMUellerNoch keine Bewertungen
- AdmimDokument2 SeitenAdmimVanessaMUellerNoch keine Bewertungen
- AssessingWounds ProcedureDokument3 SeitenAssessingWounds ProcedureVanessaMUellerNoch keine Bewertungen
- IV PushDokument3 SeitenIV PushVanessaMUeller100% (1)
- Clinical AssessementDokument2 SeitenClinical AssessementVanessaMUellerNoch keine Bewertungen
- Wound Care PDFDokument100 SeitenWound Care PDFVanessaMUellerNoch keine Bewertungen
- Example 1 - Focus: Nausea Related To AnestheticDokument1 SeiteExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerNoch keine Bewertungen
- (Chapter 3) : Cell BiologyDokument80 Seiten(Chapter 3) : Cell BiologyVanessaMUellerNoch keine Bewertungen
- Medication Guide with Side Effects and UsesDokument10 SeitenMedication Guide with Side Effects and UsesVanessaMUellerNoch keine Bewertungen
- Nurse Brain Sheet Half SizeDokument1 SeiteNurse Brain Sheet Half SizeRobyn GrogitskyNoch keine Bewertungen
- HR Ocampo Danilo s2 E10 PDFDokument4 SeitenHR Ocampo Danilo s2 E10 PDFVanessaMUellerNoch keine Bewertungen
- Indranila 2021Dokument22 SeitenIndranila 2021reski utamiNoch keine Bewertungen
- Package Insert - BOOSTRIXDokument40 SeitenPackage Insert - BOOSTRIXmiguelNoch keine Bewertungen
- Streptococcus Pneumoniae (Pneumococcus) - OverviewDokument4 SeitenStreptococcus Pneumoniae (Pneumococcus) - OverviewstarykNoch keine Bewertungen
- CB Inf HaematinicsDokument4 SeitenCB Inf Haematinicsbassam alharaziNoch keine Bewertungen
- BEmONC - Training ManualDokument263 SeitenBEmONC - Training ManualdiribaNoch keine Bewertungen
- MedVantage - Fellowship Program in Diabetes MillitusDokument2 SeitenMedVantage - Fellowship Program in Diabetes MillitusmedvantageNoch keine Bewertungen
- Guide to Bursitis Causes, Symptoms, and TreatmentDokument8 SeitenGuide to Bursitis Causes, Symptoms, and TreatmentAgeededin HartNoch keine Bewertungen
- Chapter 8A Neonatal Emergencies.Dokument35 SeitenChapter 8A Neonatal Emergencies.Sai NathNoch keine Bewertungen
- Treatment of Knee Meniscus Pathology: Rehabilitation, Surgery, and OrthobiologicsDokument17 SeitenTreatment of Knee Meniscus Pathology: Rehabilitation, Surgery, and OrthobiologicsQuiroprácticaParaTodosNoch keine Bewertungen
- MORPHINEDokument39 SeitenMORPHINEShlok RathodNoch keine Bewertungen
- Distribution of Narcotic and Other Controlled SubstancesDokument11 SeitenDistribution of Narcotic and Other Controlled SubstancesJyothsna SathpadiNoch keine Bewertungen
- Nines P Bautista, MD, MSDokument12 SeitenNines P Bautista, MD, MSadnep1991Noch keine Bewertungen
- Prelim Exam - PEC 1 Human Anatomy and PhysiologyDokument2 SeitenPrelim Exam - PEC 1 Human Anatomy and PhysiologyColeen BentoyNoch keine Bewertungen
- Medical and Surgical Emergencies Karen BallDokument62 SeitenMedical and Surgical Emergencies Karen Ballapi-195799092Noch keine Bewertungen
- CETEBE Leafleat 165x235mm 4pagesDokument2 SeitenCETEBE Leafleat 165x235mm 4pagestsveta.bozhinovaNoch keine Bewertungen
- Powerful Natural Remedies for COVID-19 and Variant StrainsDokument24 SeitenPowerful Natural Remedies for COVID-19 and Variant StrainsTracyNoch keine Bewertungen
- 9 Months Marathon Training Plan - OdtDokument6 Seiten9 Months Marathon Training Plan - OdtMichaelKahnertNoch keine Bewertungen
- Major Clinical Features of Genital Ulcers ChecklistDokument1 SeiteMajor Clinical Features of Genital Ulcers Checklistgdudex118811Noch keine Bewertungen
- K15 - Infeksi Sistem Saraf PusatDokument65 SeitenK15 - Infeksi Sistem Saraf PusatZikri Putra Lan LubisNoch keine Bewertungen
- Seddon and Sunderland Nerve Injury ClassificationDokument8 SeitenSeddon and Sunderland Nerve Injury ClassificationAndres AcostaNoch keine Bewertungen
- 3 Main Food Group: Reporter: Mercy Grace Yongco - MPA IDokument11 Seiten3 Main Food Group: Reporter: Mercy Grace Yongco - MPA ICHOSEN TABANASNoch keine Bewertungen
- Suppurative Lung DiseasesDokument39 SeitenSuppurative Lung Diseasesmatchees-gone rogueNoch keine Bewertungen
- Cga - 1Dokument19 SeitenCga - 1Kenji Tolero100% (1)