Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
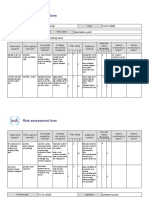
- Risk Assessment Project Iosh - MsDokument2 SeitenRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- SpiralsDokument12 SeitenSpiralskkglobalNoch keine Bewertungen
- Mathematics Specialist Unit 3A: VectorsDokument4 SeitenMathematics Specialist Unit 3A: VectorsMahir MahmoodNoch keine Bewertungen
- NSO SPRDokument9 SeitenNSO SPRADITYA SINGHNoch keine Bewertungen
- Action Plan Gulayan Sa PaaralanDokument2 SeitenAction Plan Gulayan Sa PaaralanAntonio ArienzaNoch keine Bewertungen
- Multical® 402: Data SheetDokument20 SeitenMultical® 402: Data SheetSundar RamasamyNoch keine Bewertungen
- IBH Link UA Manual PDFDokument302 SeitenIBH Link UA Manual PDFjavixl1Noch keine Bewertungen
- S120 Technical Specifications - 23 Dec 21Dokument17 SeitenS120 Technical Specifications - 23 Dec 21jayraj jadejaNoch keine Bewertungen
- SV9000 Series Products Intrduction PDFDokument90 SeitenSV9000 Series Products Intrduction PDFhamph113Noch keine Bewertungen
- Yamaha MG16 PDFDokument2 SeitenYamaha MG16 PDFmiskoyu027Noch keine Bewertungen
- TEF5-OFF Frontal Electronic TimerDokument4 SeitenTEF5-OFF Frontal Electronic TimerWhendi BmNoch keine Bewertungen
- Telmisartan, ISMNDokument8 SeitenTelmisartan, ISMNDenise EspinosaNoch keine Bewertungen
- Statistical Mechanics PDFDokument578 SeitenStatistical Mechanics PDFraymon6666100% (6)
- Civil 416Dokument2 SeitenCivil 416tskh11Noch keine Bewertungen
- NEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andDokument90 SeitenNEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andliyanderNoch keine Bewertungen
- CCNP 300 410 ENARSI NetworkTUT 26 5 2021Dokument104 SeitenCCNP 300 410 ENARSI NetworkTUT 26 5 2021Olga BradyNoch keine Bewertungen
- Zen Intro To Buddhism & Practice of ZazenDokument33 SeitenZen Intro To Buddhism & Practice of ZazendudcomeonNoch keine Bewertungen
- ASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFDokument5 SeitenASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFАртем ТитовNoch keine Bewertungen
- Starlift MetricDokument2 SeitenStarlift MetricCralesNoch keine Bewertungen
- Aerody Design of BladeDokument90 SeitenAerody Design of BladeB Bala Venkata GaneshNoch keine Bewertungen
- BookDokument28 SeitenBookFebrian Wardoyo100% (1)
- Experiment - 5Dokument26 SeitenExperiment - 5Dilip GangopadhyayNoch keine Bewertungen
- Transcendental Meditation (Four Lectures by Silo)Dokument49 SeitenTranscendental Meditation (Four Lectures by Silo)nmjoshi77859100% (2)
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDokument69 Seiten2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNoch keine Bewertungen
- Bugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54Dokument9.715 SeitenBugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54João Carlos Pereira ChoinasNoch keine Bewertungen
- Nonlinear Analysis and Optimal Design of Reinforced Concrete Plates and ShellsDokument17 SeitenNonlinear Analysis and Optimal Design of Reinforced Concrete Plates and Shellsrodain najjarNoch keine Bewertungen
- Electrical Inspections: Infrared ThermographyDokument28 SeitenElectrical Inspections: Infrared ThermographyManish RajNoch keine Bewertungen
- Gummetal Zastosowania Kliniczne 0Dokument8 SeitenGummetal Zastosowania Kliniczne 0ΑΛΕΞΑΝΔΡΟΣ ΣΤΕΦΑΝΗΣNoch keine Bewertungen
- Application of Land Suitability AnalysisDokument16 SeitenApplication of Land Suitability AnalysisHải Anh Nguyễn100% (1)
- 02 Unit I Environmental Studies-A Multidisciplinary Subject 14-01-2022Dokument69 Seiten02 Unit I Environmental Studies-A Multidisciplinary Subject 14-01-2022doramonbhaiyaNoch keine Bewertungen