Das könnte Ihnen auch gefallen
- Selection of Implants in Vogue: Dr.D.J. ArwadeDokument15 SeitenSelection of Implants in Vogue: Dr.D.J. Arwadedoctorsuril9108Noch keine Bewertungen
- QUT Digital RepositoryDokument6 SeitenQUT Digital RepositoryShofia MoehNoch keine Bewertungen
- ETN TecnicaDokument92 SeitenETN TecnicaJorge JesusNoch keine Bewertungen
- Mini-Implant Anchorage For The Orthodontic Practitioner PDFDokument7 SeitenMini-Implant Anchorage For The Orthodontic Practitioner PDFkjunaidNoch keine Bewertungen
- Lock Distal Radius SystemDokument20 SeitenLock Distal Radius SystemBilal AhmadNoch keine Bewertungen
- Instrumen Endodontik PatahDokument8 SeitenInstrumen Endodontik PatahKhamila TusyNoch keine Bewertungen
- Introduction To Dental Implants 2017 PDFDokument61 SeitenIntroduction To Dental Implants 2017 PDFChong Weng Wah100% (2)
- Various Treatment Modalities For Retrieval of Broken Abutment Screw in Implant ProsthodonticsDokument6 SeitenVarious Treatment Modalities For Retrieval of Broken Abutment Screw in Implant Prosthodonticsrood_kNoch keine Bewertungen
- ORP Handout English External Fixation NlogoDokument9 SeitenORP Handout English External Fixation NlogotripodegrandeNoch keine Bewertungen
- Retrieval of Fractured Abutment Screw From The Implant 2Dokument27 SeitenRetrieval of Fractured Abutment Screw From The Implant 2nadeemNoch keine Bewertungen
- Removal of A Broken Distal Closed Section Intramedullary NailDokument3 SeitenRemoval of A Broken Distal Closed Section Intramedullary Nailratnav_ratanNoch keine Bewertungen
- 200810110-112 Innova ArticleDokument2 Seiten200810110-112 Innova ArticleMery MerryNoch keine Bewertungen
- Dental Implant: Presented byDokument43 SeitenDental Implant: Presented byade ismailNoch keine Bewertungen
- Fracture Fixation - Interlocking Nail Technique in Dogs - Vetlexicon Canis From Vetstream - Definitive Veterinary IntelligenceDokument4 SeitenFracture Fixation - Interlocking Nail Technique in Dogs - Vetlexicon Canis From Vetstream - Definitive Veterinary IntelligencePrabhu KumarNoch keine Bewertungen
- ZNN Retrograde NailDokument24 SeitenZNN Retrograde Nailmisterx73Noch keine Bewertungen
- Large Medium ExternalfixatorsDokument42 SeitenLarge Medium ExternalfixatorsZulfadli Salleh0% (1)
- MUCLecture 2022 82714630Dokument7 SeitenMUCLecture 2022 82714630Muthoni EliasNoch keine Bewertungen
- PIIS0022391322004668Dokument9 SeitenPIIS0022391322004668LalaNoch keine Bewertungen
- English Screws HandoutDokument10 SeitenEnglish Screws HandouteugenetbkNoch keine Bewertungen
- Gamma NailDokument49 SeitenGamma NailMihaela HerghelegiuNoch keine Bewertungen
- Stryker Variax Fibula OTDokument24 SeitenStryker Variax Fibula OTDan IonescuNoch keine Bewertungen
- Temporary Anchorage Devices in Orthodont 970c9d2aDokument11 SeitenTemporary Anchorage Devices in Orthodont 970c9d2aThang Nguyen TienNoch keine Bewertungen
- Review of Implant SystemsDokument41 SeitenReview of Implant Systemsjojiimplant100% (2)
- An Unconventional Approach For Retrieval of Fractured Prosthetic Screw A Case ReportDokument4 SeitenAn Unconventional Approach For Retrieval of Fractured Prosthetic Screw A Case ReportBagis Emre GulNoch keine Bewertungen
- Removal of Stuck Femur Interlocking Nail by Longitudinal Osteotomy of Femur - A Case ReportDokument4 SeitenRemoval of Stuck Femur Interlocking Nail by Longitudinal Osteotomy of Femur - A Case ReportIJAR JOURNALNoch keine Bewertungen
- Post Graduate Student: Dr. RahultiwariDokument158 SeitenPost Graduate Student: Dr. RahultiwariVivek Sunil EdayathNoch keine Bewertungen
- Gamma LungDokument52 SeitenGamma LungOana AlexandraNoch keine Bewertungen
- 3 To 7 Years Longit Study 2004Dokument6 Seiten3 To 7 Years Longit Study 2004Hicham AL KHAYARNoch keine Bewertungen
- DR Ghazy 2013 Implant Lectures For 4th Year StudentsDokument25 SeitenDR Ghazy 2013 Implant Lectures For 4th Year StudentsMohamed Hamed GhazyNoch keine Bewertungen
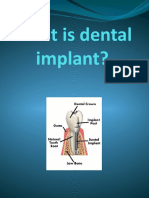
- What Is Dental ImplantDokument14 SeitenWhat Is Dental ImplantFaleh ZahrawiNoch keine Bewertungen
- Retrograde Removal of Broken Intra Medullary Femoral Nail An Innovative TechniqueDokument3 SeitenRetrograde Removal of Broken Intra Medullary Femoral Nail An Innovative TechniqueArsalan BukhariNoch keine Bewertungen
- Precision Attachments (2) PRDokument23 SeitenPrecision Attachments (2) PRpriyaNoch keine Bewertungen
- Removing Bridge PDFDokument6 SeitenRemoving Bridge PDFElbanus WatriNoch keine Bewertungen
- Complications and Maintenance of Dental ImplantDokument5 SeitenComplications and Maintenance of Dental ImplantAkshay GajakoshNoch keine Bewertungen
- Articulo 2 EndoDokument11 SeitenArticulo 2 EndoPedro Gonzalez DelgadoNoch keine Bewertungen
- ImplantDokument9 SeitenImplantKhaled Abo ZaidNoch keine Bewertungen
- Management Mandible ReconstructionsDokument32 SeitenManagement Mandible ReconstructionsHidayatNoch keine Bewertungen
- Cancanous Screw TechguideDokument12 SeitenCancanous Screw TechguideĐức LộcNoch keine Bewertungen
- Implant Removal After Intramedullary Osteosyntheses. Literature Review, Technical Details, and Tips and TricksDokument1 SeiteImplant Removal After Intramedullary Osteosyntheses. Literature Review, Technical Details, and Tips and TricksFrancesco RugoloNoch keine Bewertungen
- Attachment Procedures: Attachments in DentistryDokument7 SeitenAttachment Procedures: Attachments in DentistryRohan GroverNoch keine Bewertungen
- Retrospective Study On Efficacy of Intermaxillary Fixation ScrewsDokument3 SeitenRetrospective Study On Efficacy of Intermaxillary Fixation ScrewsPorcupine TreeNoch keine Bewertungen
- Intracoronal Attachments For Removable Partial DenturesDokument18 SeitenIntracoronal Attachments For Removable Partial Denturesapi-3710948100% (6)
- Module 6-5 Fasteners Pt4 PresentationDokument46 SeitenModule 6-5 Fasteners Pt4 Presentationabdullahqureshi789456Noch keine Bewertungen
- SUTGTielas LJ3231 HDokument38 SeitenSUTGTielas LJ3231 HAndreea ChiriloiuNoch keine Bewertungen
- Nut (Hardware) - Wikipedia, The Free EncyclopediaDokument6 SeitenNut (Hardware) - Wikipedia, The Free EncyclopediashivarwatNoch keine Bewertungen
- Engineering Drawing - Fastening Devices Research PaperDokument16 SeitenEngineering Drawing - Fastening Devices Research PaperMalik ForbesNoch keine Bewertungen
- Removal of Hardware BlogDokument5 SeitenRemoval of Hardware BlogJill McAngusNoch keine Bewertungen
- Splinting of Teeth Following TraumaDokument73 SeitenSplinting of Teeth Following TraumaSHRINIVAS GARJENoch keine Bewertungen
- Splinting of Teeth Following TraumaDokument73 SeitenSplinting of Teeth Following TraumaSHRINIVAS GARJENoch keine Bewertungen
- Precision AttachmentsDokument10 SeitenPrecision Attachmentsdentist40Noch keine Bewertungen
- IMPLANTSDokument24 SeitenIMPLANTSHarsh PawarNoch keine Bewertungen
- 1158 PDFDokument7 Seiten1158 PDFankitaNoch keine Bewertungen
- External FixationDokument4 SeitenExternal FixationZilbran BerontaxNoch keine Bewertungen
- Imp 1Dokument5 SeitenImp 1pradeepgade1Noch keine Bewertungen
- Fixed Orthodontic Appliances: A Practical GuideVon EverandFixed Orthodontic Appliances: A Practical GuideBewertung: 1 von 5 Sternen1/5 (1)
- Short ImplantsVon EverandShort ImplantsBoyd J. TomasettiNoch keine Bewertungen
- 2012 Article 202Dokument12 Seiten2012 Article 202cronoss21Noch keine Bewertungen
- Femoral Nonunion - Risk Factors and Treatment Options PDFDokument10 SeitenFemoral Nonunion - Risk Factors and Treatment Options PDFcronoss21Noch keine Bewertungen
- Regenerative Medicine For The Musculoskeletal System Based On Muscle-Derived Stem CellsDokument9 SeitenRegenerative Medicine For The Musculoskeletal System Based On Muscle-Derived Stem Cellscronoss21Noch keine Bewertungen
- Gender-Specific Knee Replacements - A Technology OverviewDokument5 SeitenGender-Specific Knee Replacements - A Technology Overviewcronoss21Noch keine Bewertungen
- Unicompartmental Knee ArthroplastyDokument10 SeitenUnicompartmental Knee Arthroplastycronoss21Noch keine Bewertungen
- Cast and Splint Immobilization - Complications PDFDokument11 SeitenCast and Splint Immobilization - Complications PDFcronoss21Noch keine Bewertungen
- Psychiatric Aspects of OrthopaedicsDokument6 SeitenPsychiatric Aspects of Orthopaedicscronoss21Noch keine Bewertungen
- Borderou RezidentiatDokument1 SeiteBorderou Rezidentiatluci_wyvern1390950% (4)
- Xenotransplantation in Orthopaedic SurgeryDokument5 SeitenXenotransplantation in Orthopaedic Surgerycronoss21Noch keine Bewertungen
- Cervical LaminaplastyDokument10 SeitenCervical Laminaplastycronoss21Noch keine Bewertungen
- Culegere Grile Rezidentiat 2013Dokument764 SeitenCulegere Grile Rezidentiat 2013Simona IonitaNoch keine Bewertungen
- Resuscitare 2014Dokument79 SeitenResuscitare 2014cronoss21Noch keine Bewertungen
- Infectii Virale Feb2014Dokument81 SeitenInfectii Virale Feb2014cronoss21Noch keine Bewertungen
- Office 2007 SerialDokument1 SeiteOffice 2007 Serialnicu_consta89Noch keine Bewertungen
- MU - Acoplamiento MidasRex AA10, AF02Dokument232 SeitenMU - Acoplamiento MidasRex AA10, AF02Javi Payá HerrerosNoch keine Bewertungen
- Corner Back DrillsDokument16 SeitenCorner Back DrillsDrew43stl100% (1)
- Genital Tract InjuriesDokument19 SeitenGenital Tract InjuriesMarvella Nongkhar100% (1)
- Types of Wounds 101Dokument17 SeitenTypes of Wounds 101Grey Tapes100% (1)
- Blunt Force TraumaDokument19 SeitenBlunt Force TraumaIna KeyserNoch keine Bewertungen
- Integumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageDokument6 SeitenIntegumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageGabrielitoNoch keine Bewertungen
- Emergency Acute and Rapid Access Ophthalmology Practical, Clinical and Managerial AspectsDokument137 SeitenEmergency Acute and Rapid Access Ophthalmology Practical, Clinical and Managerial Aspectsvirus100% (1)
- Trauma VascularDokument30 SeitenTrauma Vascularblip blip blooop0% (2)
- NEET PG 2015 Question Paper With SolutionsDokument1.852 SeitenNEET PG 2015 Question Paper With SolutionsSK RaulNoch keine Bewertungen
- WAR Chip - ManualDokument26 SeitenWAR Chip - Manualjosh_astrologoNoch keine Bewertungen
- Underwater Blast InjuriesDokument10 SeitenUnderwater Blast Injuriestonylee24Noch keine Bewertungen
- Morariu DDDprelimASN (1) (Compatibility Mode)Dokument25 SeitenMorariu DDDprelimASN (1) (Compatibility Mode)SAKSHI KATIYARNoch keine Bewertungen
- Laboratory Manual For Anatomy and Physiology 6Th Edition Marieb Solutions Manual Full Chapter PDFDokument28 SeitenLaboratory Manual For Anatomy and Physiology 6Th Edition Marieb Solutions Manual Full Chapter PDFJohnathanFitzgeraldnwoa100% (10)
- PC 3.3 With QSK45 and 60Dokument432 SeitenPC 3.3 With QSK45 and 60Sajid Hanif91% (11)
- Atls Trauma ThermalDokument36 SeitenAtls Trauma ThermalsheisamarinkaNoch keine Bewertungen
- Principles of Oral SurgeryDokument56 SeitenPrinciples of Oral SurgeryJayeshNoch keine Bewertungen
- Pain and Effusion and Quadriceps Activation and StrengthDokument6 SeitenPain and Effusion and Quadriceps Activation and StrengthЯнь НгуенNoch keine Bewertungen
- Sergio Amonoy Vs Spouses GutierrezDokument1 SeiteSergio Amonoy Vs Spouses GutierrezshamymyNoch keine Bewertungen
- Positioning and Drafting ReviewerDokument4 SeitenPositioning and Drafting ReviewerKathrina Mendoza HembradorNoch keine Bewertungen
- IntroductionDokument35 SeitenIntroductionBhaktiNoch keine Bewertungen
- Understanding The Trauma Activation FeeDokument7 SeitenUnderstanding The Trauma Activation Feenlprofits100% (1)
- Gait AsessmentDokument57 SeitenGait Asessmentsurender_singh_43Noch keine Bewertungen
- Skin Wounds Vitality Markers in Forensic Pathology - An Updated ReviewDokument10 SeitenSkin Wounds Vitality Markers in Forensic Pathology - An Updated Reviewrodrigo100% (1)
- Makka Ho StretchesDokument4 SeitenMakka Ho Stretchesdianaazzam2100% (3)
- Keith L. Moore - A. M. R. Agur - II Arthur F. Dalley - Keith L. Moore - Moore's Essential Clinical Anatomy (2019) - 120Dokument1 SeiteKeith L. Moore - A. M. R. Agur - II Arthur F. Dalley - Keith L. Moore - Moore's Essential Clinical Anatomy (2019) - 120arditia dwiNoch keine Bewertungen
- A Joint by Joint Approach To TrainingDokument5 SeitenA Joint by Joint Approach To TrainingLloydNoch keine Bewertungen
- Articular Neurophysiology: Presented by - Yogesh VyasDokument15 SeitenArticular Neurophysiology: Presented by - Yogesh VyasvictoryvelavaNoch keine Bewertungen
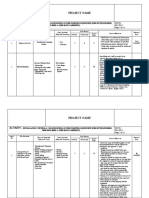
- Riask Assessment FF Equipment Installation & TestingDokument11 SeitenRiask Assessment FF Equipment Installation & Testingbeho2000100% (1)
- Oblivion by Anthony Horowitz Sample ChapterDokument17 SeitenOblivion by Anthony Horowitz Sample ChapterWalker Books100% (4)