Das könnte Ihnen auch gefallen
- Mohammad Aqel CVDokument1 SeiteMohammad Aqel CVMohammad AqelNoch keine Bewertungen
- Cover LetterDokument2 SeitenCover LetterMohammad AqelNoch keine Bewertungen
- Vertical CurvesDokument8 SeitenVertical CurvesRJay DorojaNoch keine Bewertungen
- Diaphragm WallDokument28 SeitenDiaphragm WallTiong V YenNoch keine Bewertungen
- Bubble DeckDokument16 SeitenBubble Deckdeepuvarghese100% (1)
- Pile FoundationDokument10 SeitenPile FoundationMohammad AqelNoch keine Bewertungen
- Statement For ApplicationDokument1 SeiteStatement For ApplicationMohammad AqelNoch keine Bewertungen
- Computer Aided Engineering Drawing: Arch. Oraib A. Al-JaafrehDokument29 SeitenComputer Aided Engineering Drawing: Arch. Oraib A. Al-JaafrehMohammad AqelNoch keine Bewertungen
- ResumeDokument1 SeiteResumeSteven ObrienNoch keine Bewertungen
- هندسة مرورDokument6 Seitenهندسة مرورMohammad AqelNoch keine Bewertungen
- - كتاب شرح الكود الامريكى بالعربىDokument345 Seiten- كتاب شرح الكود الامريكى بالعربىMohamed Abbassy88% (26)
- تعديل2Dokument20 Seitenتعديل2Mohammad AqelNoch keine Bewertungen
- Problem 2 SolutionDokument2 SeitenProblem 2 SolutionMohammad AqelNoch keine Bewertungen
- Angle Measurements: - ConversionsDokument14 SeitenAngle Measurements: - ConversionsMohammad AqelNoch keine Bewertungen
- Cut-N-Fill 1 14Dokument64 SeitenCut-N-Fill 1 14Mohammad AqelNoch keine Bewertungen
- Earthwork and Mass Diagram 1Dokument39 SeitenEarthwork and Mass Diagram 1Mohammad Aqel100% (1)
- GpsDokument43 SeitenGpsMohammad AqelNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Food TechDokument41 SeitenFood TechMD Ishteyaque AhmadNoch keine Bewertungen
- Electronegativity (Allen Scale)Dokument2 SeitenElectronegativity (Allen Scale)YourMotherNoch keine Bewertungen
- Astm A1078Dokument5 SeitenAstm A1078mmendez11333% (3)
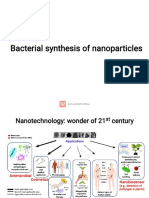
- Bacterial SynthesisDokument16 SeitenBacterial SynthesisDibyajyoti20 Das4001Noch keine Bewertungen
- Revised 4th Sem Time Table - FDokument5 SeitenRevised 4th Sem Time Table - FJerry boyNoch keine Bewertungen
- Physics II Problems PDFDokument1 SeitePhysics II Problems PDFBOSS BOSSNoch keine Bewertungen
- m3 CalculationDokument45 Seitenm3 CalculationHgagselim Selim100% (1)
- Casein Hydrolysis by Immobilized Enzymes in A Torus ReactorDokument7 SeitenCasein Hydrolysis by Immobilized Enzymes in A Torus ReactorLia NashNoch keine Bewertungen
- Materials Science & Engineering B: SciencedirectDokument10 SeitenMaterials Science & Engineering B: SciencedirectMuhammad BramansyahNoch keine Bewertungen
- First Quarter Examination in Science ViDokument2 SeitenFirst Quarter Examination in Science ViRODELITO ARAMAYNoch keine Bewertungen
- Daftar Pustaka KilnDokument2 SeitenDaftar Pustaka Kilnazzahra ghina fadillahNoch keine Bewertungen
- Determination of Specific Gravity: Experiment No 2 Soil Mechanics Laboratory CE PC 594Dokument11 SeitenDetermination of Specific Gravity: Experiment No 2 Soil Mechanics Laboratory CE PC 594SumanHaldarNoch keine Bewertungen
- Heavy Metal Removal From Water Using Moringa Oleifera Seed Coagulant and Double FiltrationDokument4 SeitenHeavy Metal Removal From Water Using Moringa Oleifera Seed Coagulant and Double FiltrationAena RabonzaNoch keine Bewertungen
- Oxy GraphDokument2 SeitenOxy Graphdavid_physiologyNoch keine Bewertungen
- Experimento de Anfisen en Pliegues de Proteina (Articulo Original)Dokument9 SeitenExperimento de Anfisen en Pliegues de Proteina (Articulo Original)Exe bolsilludoNoch keine Bewertungen
- Epikure Curing Agent 05443 - Eu - enDokument17 SeitenEpikure Curing Agent 05443 - Eu - enanacarol09Noch keine Bewertungen
- Uni ConveyerDokument88 SeitenUni Conveyerapi-26356646Noch keine Bewertungen
- 2-Excellent Chemistry Assignment The Solid StatesDokument5 Seiten2-Excellent Chemistry Assignment The Solid StatesSachin B SNoch keine Bewertungen
- Nabakem PCB Insulating Coating AgentDokument4 SeitenNabakem PCB Insulating Coating Agentsutrisno00Noch keine Bewertungen
- Catalog Biocraft Electronic Test InstrumentDokument2 SeitenCatalog Biocraft Electronic Test InstrumentHmmNoch keine Bewertungen
- Two Solid Cylindrical Rods AB and 2. Select The Appropriate Pair of ElementsDokument4 SeitenTwo Solid Cylindrical Rods AB and 2. Select The Appropriate Pair of ElementsAhmed Dhempsey Hali AbdulbasikNoch keine Bewertungen
- Model QAP For Plates1Dokument3 SeitenModel QAP For Plates1tarun kaushalNoch keine Bewertungen
- AFT Arrow 5 Data Sheet PDFDokument2 SeitenAFT Arrow 5 Data Sheet PDFerjainrachitNoch keine Bewertungen
- Report For Experiment #21 Radioactive Decay: Monique DesrochersDokument9 SeitenReport For Experiment #21 Radioactive Decay: Monique DesrochersMonique DesrochersNoch keine Bewertungen
- LC Training Basic HPLC 2001 ADokument124 SeitenLC Training Basic HPLC 2001 Abile86Noch keine Bewertungen
- Nonvolatile Content of Varnishes: Standard Test Methods ForDokument2 SeitenNonvolatile Content of Varnishes: Standard Test Methods ForGiovanni OsorioNoch keine Bewertungen
- Unit-I Chemical Bonding and Molecular Structure: (18 Contact Hours)Dokument3 SeitenUnit-I Chemical Bonding and Molecular Structure: (18 Contact Hours)Imran Afzal BhatNoch keine Bewertungen
- 15 PDFDokument28 Seiten15 PDFNathanNoch keine Bewertungen
- Specifications of Nitofill EPLV PDFDokument2 SeitenSpecifications of Nitofill EPLV PDFTrung Nguyen ThanhNoch keine Bewertungen