Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Experience of Health Professionals Around An Exorcism: A Case ReportDokument4 SeitenExperience of Health Professionals Around An Exorcism: A Case ReportsorinfNoch keine Bewertungen
- Dyslexia and DyscalculiaDokument15 SeitenDyslexia and DyscalculiaSarah BaczanskiNoch keine Bewertungen
- Future of The Pharmaceutical Industry in The GCC 2017 PDFDokument3 SeitenFuture of The Pharmaceutical Industry in The GCC 2017 PDFJeet MehtaNoch keine Bewertungen
- All India Network Hospitals GeneralDokument630 SeitenAll India Network Hospitals GeneralPankajNoch keine Bewertungen
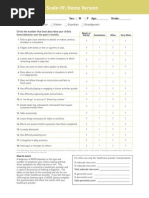
- Screening ADHDDokument2 SeitenScreening ADHDPsiholog Alina Mirela CraiuNoch keine Bewertungen
- Mo2vate Issue 15 - March 2022Dokument74 SeitenMo2vate Issue 15 - March 2022Mo2vate MagazineNoch keine Bewertungen
- HIV/AIDS Education GuideDokument12 SeitenHIV/AIDS Education GuideDutch EarthNoch keine Bewertungen
- Shulbi@merseta.o RG - Za 010 219 3367Dokument111 SeitenShulbi@merseta.o RG - Za 010 219 3367Michael NcubeNoch keine Bewertungen
- GMC Handwara Recruitment 2023Dokument4 SeitenGMC Handwara Recruitment 2023Ummar WaniNoch keine Bewertungen
- The China Study Diiet Plan - MP TiwariDokument3 SeitenThe China Study Diiet Plan - MP Tiwarirajanlko100% (1)
- Meditation and Energy HealingDokument16 SeitenMeditation and Energy HealingCristian CatalinaNoch keine Bewertungen
- Infection Control: Principles in Medical Laboratory Science Practice 1Dokument10 SeitenInfection Control: Principles in Medical Laboratory Science Practice 1Greggory John Tiu CequiñaNoch keine Bewertungen
- FW02 Phy ActivitiesDokument13 SeitenFW02 Phy Activitiesjojo basenNoch keine Bewertungen
- The Prevalence of Malaria Among Pregnant Women On Addmission in Imo State Specialist Hospital OwerriDokument34 SeitenThe Prevalence of Malaria Among Pregnant Women On Addmission in Imo State Specialist Hospital OwerriDaniel ObasiNoch keine Bewertungen
- Learners Individual Reading Assessment ToolDokument7 SeitenLearners Individual Reading Assessment ToolMhen AcenasNoch keine Bewertungen
- XII EnglishDokument11 SeitenXII EnglishNancy GautamNoch keine Bewertungen
- Blood Pressure Variability: How To Deal?: NR Rau, Gurukanth RaoDokument5 SeitenBlood Pressure Variability: How To Deal?: NR Rau, Gurukanth RaoRully SyahrizalNoch keine Bewertungen
- Regulatory Bodies of Nursing in India: Dr. Maheswari JaikumarDokument75 SeitenRegulatory Bodies of Nursing in India: Dr. Maheswari Jaikumarkalla sharonNoch keine Bewertungen
- Cataract PTDokument9 SeitenCataract PTPreeti SharmaNoch keine Bewertungen
- Personal Development 11 Q1 LAS Week4Dokument8 SeitenPersonal Development 11 Q1 LAS Week4Ruben100% (1)
- MSDS Ultrachem Bond AcrDokument5 SeitenMSDS Ultrachem Bond Acrjohan tindiNoch keine Bewertungen
- Tor WFP Food Assistance For Assets ProjectDokument15 SeitenTor WFP Food Assistance For Assets Projectsabri HanshiNoch keine Bewertungen
- Project Management Contractor Wellness Report: Saudi Aramco: Company General UseDokument1 SeiteProject Management Contractor Wellness Report: Saudi Aramco: Company General UseSabre AlamNoch keine Bewertungen
- Breastfeeding ManagementDokument12 SeitenBreastfeeding ManagementtitisNoch keine Bewertungen
- Paramyxovir Idae: Disease/Viral FactorsDokument22 SeitenParamyxovir Idae: Disease/Viral FactorsMary ChristelleNoch keine Bewertungen
- Cancer Bathinda's Dubious DistinctionDokument2 SeitenCancer Bathinda's Dubious DistinctionPardeepSinghNoch keine Bewertungen
- VutaminDokument66 SeitenVutamindyla nabillaNoch keine Bewertungen
- Doh NOTES-1Dokument196 SeitenDoh NOTES-1norabilbaoNoch keine Bewertungen
- Aspek Etik Dan Legal Dalam Keperawatan BencanaDokument11 SeitenAspek Etik Dan Legal Dalam Keperawatan BencanaPhiioNoch keine Bewertungen
- Presentation by DR Madhur Rai - Case Studies of Patients Practising Sahaja Yoga MeditationDokument16 SeitenPresentation by DR Madhur Rai - Case Studies of Patients Practising Sahaja Yoga Meditationtanaha100% (3)