Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- ROA Salmonella-Enteritidis-ST11 2022 FinalDokument19 SeitenROA Salmonella-Enteritidis-ST11 2022 FinalFrancisca BallesterosNoch keine Bewertungen
- 5communicable Disease Threats Report 30 Jul 2022 PublicDokument28 Seiten5communicable Disease Threats Report 30 Jul 2022 PublicFrancisca BallesterosNoch keine Bewertungen
- 2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeDokument11 Seiten2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeFrancisca BallesterosNoch keine Bewertungen
- 3interim Advice For Public Health Authorities On Summer Events MPXDokument6 Seiten3interim Advice For Public Health Authorities On Summer Events MPXFrancisca BallesterosNoch keine Bewertungen
- 1considerations For Contact Tracing MPX June 2022Dokument13 Seiten1considerations For Contact Tracing MPX June 2022Francisca BallesterosNoch keine Bewertungen
- Joint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Dokument7 SeitenJoint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Francisca BallesterosNoch keine Bewertungen
- 2021-01-13 Variable Dictionary and Disclaimer National Weekly DataDokument1 Seite2021-01-13 Variable Dictionary and Disclaimer National Weekly DataFrancisca BallesterosNoch keine Bewertungen
- Interim Public Health Considerations For COVID 19 Vaccination of AdolescentsDokument19 SeitenInterim Public Health Considerations For COVID 19 Vaccination of AdolescentsFrancisca BallesterosNoch keine Bewertungen
- Variable Dictionary VaccineTracker-04!11!2021Dokument3 SeitenVariable Dictionary VaccineTracker-04!11!2021Francisca BallesterosNoch keine Bewertungen
- COVID 19 in Children and The Role of School Settings in Transmission Second UpdateDokument37 SeitenCOVID 19 in Children and The Role of School Settings in Transmission Second UpdateFrancisca BallesterosNoch keine Bewertungen
- Description and Disclaimer Daily ReportingDokument1 SeiteDescription and Disclaimer Daily ReportingFrancisca BallesterosNoch keine Bewertungen
- ECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEADokument1 SeiteECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEAFrancisca BallesterosNoch keine Bewertungen
- Use of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesDokument5 SeitenUse of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesFrancisca BallesterosNoch keine Bewertungen
- COVID 19 Considerations For Booster Doses in Adolescents Feb 2022Dokument14 SeitenCOVID 19 Considerations For Booster Doses in Adolescents Feb 2022Francisca BallesterosNoch keine Bewertungen
- Zika Virus Safety of Substances of Human Origin Update 2017 WebDokument35 SeitenZika Virus Safety of Substances of Human Origin Update 2017 WebFrancisca BallesterosNoch keine Bewertungen
- Hiv and Aids: Surveillance ReportDokument7 SeitenHiv and Aids: Surveillance ReportFrancisca BallesterosNoch keine Bewertungen
- Variable Dictionary VaccineTracker-20-08-2021Dokument3 SeitenVariable Dictionary VaccineTracker-20-08-2021Francisca BallesterosNoch keine Bewertungen
- Communicable Disease Threats Report 26 Aug 2017Dokument9 SeitenCommunicable Disease Threats Report 26 Aug 2017Francisca BallesterosNoch keine Bewertungen
- Antimicrobial Resistance Europe 2015Dokument120 SeitenAntimicrobial Resistance Europe 2015Francisca BallesterosNoch keine Bewertungen
- Agenda EAAD - European-Level Launch EventDokument1 SeiteAgenda EAAD - European-Level Launch EventFrancisca BallesterosNoch keine Bewertungen
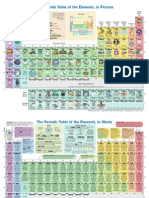
- The Periodic Table of Elements, in PicturesDokument2 SeitenThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- Communicable Disease Threats Report 29 Jul 2017Dokument13 SeitenCommunicable Disease Threats Report 29 Jul 2017Francisca BallesterosNoch keine Bewertungen
- Who Ccsivd Meetingreport SangreDokument31 SeitenWho Ccsivd Meetingreport SangreFrancisca BallesterosNoch keine Bewertungen
- Communicable Disease Threats Report 16 Jun 2018Dokument11 SeitenCommunicable Disease Threats Report 16 Jun 2018Francisca BallesterosNoch keine Bewertungen
- Ecdc Infographics2015 Measles Is SeriousDokument1 SeiteEcdc Infographics2015 Measles Is SeriousFrancisca BallesterosNoch keine Bewertungen
- ECDC - ECDC Policy Briefing - Preparing For Zika in The EUDokument1 SeiteECDC - ECDC Policy Briefing - Preparing For Zika in The EUFrancisca BallesterosNoch keine Bewertungen
- ECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyDokument1 SeiteECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyFrancisca BallesterosNoch keine Bewertungen
- ECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsDokument2 SeitenECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsFrancisca BallesterosNoch keine Bewertungen
- ECDC Policy BriefingsDokument1 SeiteECDC Policy BriefingsFrancisca BallesterosNoch keine Bewertungen
- ECDC Epidemiological SituationDokument1 SeiteECDC Epidemiological SituationFrancisca BallesterosNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Manual Jib 25 10 02Dokument256 SeitenManual Jib 25 10 02Luis Jose LlobanNoch keine Bewertungen
- Doka H20 BeamDokument20 SeitenDoka H20 Beamshoaib100% (1)
- Review Related LiteratureDokument3 SeitenReview Related LiteratureHanz EspirituNoch keine Bewertungen
- Conceptual Design and Development of Shredding Machine For Agricultural WasteDokument7 SeitenConceptual Design and Development of Shredding Machine For Agricultural WasteVJ CarbonellNoch keine Bewertungen
- H1.001858 Strongpack Nigeria-Electrical Loads List For Layout Utilities-Rev-02Dokument1 SeiteH1.001858 Strongpack Nigeria-Electrical Loads List For Layout Utilities-Rev-02yseffoNoch keine Bewertungen
- Colonel SandersDokument17 SeitenColonel SandersAmandaNoch keine Bewertungen
- Extubation After Difficult IntubationDokument3 SeitenExtubation After Difficult Intubationramanrajesh83Noch keine Bewertungen
- Answers To Competency Assessment SectionDokument16 SeitenAnswers To Competency Assessment Sectionapi-209542414100% (1)
- PU-133AB - 規格GMXa spc 2022Dokument5 SeitenPU-133AB - 規格GMXa spc 2022Ý TrầnNoch keine Bewertungen
- User's Manual Eco Friendly Park BenchDokument35 SeitenUser's Manual Eco Friendly Park BenchAmirulHanif AlyahyaNoch keine Bewertungen
- Clay Analysis - 1Dokument55 SeitenClay Analysis - 1JCSNoch keine Bewertungen
- Medical Gases: NO. Item Brand Name OriginDokument4 SeitenMedical Gases: NO. Item Brand Name OriginMahmoud AnwerNoch keine Bewertungen
- 1635 The Papal Stakes - Eric FlintDokument1.813 Seiten1635 The Papal Stakes - Eric Flintwon100% (2)
- ChartDokument27 SeitenChartFlorijan ŠafarNoch keine Bewertungen
- Oxigen Gen Container CMM 35-21-14Dokument151 SeitenOxigen Gen Container CMM 35-21-14herrisutrisna100% (2)
- Paracetamol DegradationDokument9 SeitenParacetamol DegradationTruyền Phạm MinhNoch keine Bewertungen
- 2457-Article Text-14907-2-10-20120724Dokument6 Seiten2457-Article Text-14907-2-10-20120724desi meleniaNoch keine Bewertungen
- 50-Article Text-116-1-10-20191113Dokument6 Seiten50-Article Text-116-1-10-20191113Annisa FauziahNoch keine Bewertungen
- Technical Reference For Water Conservation in Cooling TowersDokument41 SeitenTechnical Reference For Water Conservation in Cooling TowersDorn GalamarNoch keine Bewertungen
- Hydraulic Fluid CategoriesDokument3 SeitenHydraulic Fluid CategoriesJako MishyNoch keine Bewertungen
- Test Unit 2 Urbanisation L P 12Dokument9 SeitenTest Unit 2 Urbanisation L P 12Xuân NguyenNoch keine Bewertungen
- EDU403 Assignment 1Dokument6 SeitenEDU403 Assignment 1NadiaJawadHussainNoch keine Bewertungen
- Vishaka GuidelinesDokument4 SeitenVishaka GuidelinesAakashKumarNoch keine Bewertungen
- A - S-2W & B - S-2W Series: 2W, Fixed Input, Isolated & Unregulated Dual/Single Output DC-DC ConverterDokument5 SeitenA - S-2W & B - S-2W Series: 2W, Fixed Input, Isolated & Unregulated Dual/Single Output DC-DC ConverteranonbeatNoch keine Bewertungen
- All About Ocean Life-Rachel BladonDokument6 SeitenAll About Ocean Life-Rachel BladonRichard TekulaNoch keine Bewertungen
- Manual GISDokument36 SeitenManual GISDanil Pangestu ChandraNoch keine Bewertungen
- Piaget and Preoperational StageDokument2 SeitenPiaget and Preoperational Stageapi-285179229Noch keine Bewertungen
- Calamity and Disaster Preparedness Chapter IXDokument34 SeitenCalamity and Disaster Preparedness Chapter IXANGEL ALBERTNoch keine Bewertungen
- Ragin Cajun PDFDokument2 SeitenRagin Cajun PDFjosemfcNoch keine Bewertungen
- Hand-Pallet Truck - NewDokument2 SeitenHand-Pallet Truck - NewAkhilNoch keine Bewertungen