Das könnte Ihnen auch gefallen
- Management of Cirrhosis of The LiverDokument48 SeitenManagement of Cirrhosis of The LiverksofianaNoch keine Bewertungen
- Chronic Liver Diseases & PLCCDokument56 SeitenChronic Liver Diseases & PLCCibnbasheer100% (5)
- Viral Hepatitis: A C EDokument47 SeitenViral Hepatitis: A C EgigibesiNoch keine Bewertungen
- Viral HepatitisDokument64 SeitenViral Hepatitisapi-19916399Noch keine Bewertungen
- Hepatitis & It's ComplicationDokument11 SeitenHepatitis & It's ComplicationHadjar Mingfan FlamerNoch keine Bewertungen
- Jaundice and HepatitisDokument7 SeitenJaundice and Hepatitismariam saqibNoch keine Bewertungen
- 1 HepatitisDokument22 Seiten1 Hepatitissara.sherif099Noch keine Bewertungen
- Hepatits: Nitha K 2nd Year MSC NursingDokument88 SeitenHepatits: Nitha K 2nd Year MSC NursingNITHA KNoch keine Bewertungen
- Acute HepatitisDokument34 SeitenAcute HepatitisThoma KumaraNoch keine Bewertungen
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDokument35 SeitenLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNoch keine Bewertungen
- 8 - Git2 'Dokument44 Seiten8 - Git2 'ALNAKINoch keine Bewertungen
- Askep SirosisDokument73 SeitenAskep SirosisRisma Yuliana PratiwiNoch keine Bewertungen
- The Liver - The Bil - TR.,V, UNUD, 2019Dokument76 SeitenThe Liver - The Bil - TR.,V, UNUD, 2019Wilson HalimNoch keine Bewertungen
- Overview of HepatopathologyDokument158 SeitenOverview of Hepatopathologyamy100% (1)
- GIT Portal HypertensionDokument24 SeitenGIT Portal HypertensionDr.P.NatarajanNoch keine Bewertungen
- Sirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSDokument66 SeitenSirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSArif Rahman DmNoch keine Bewertungen
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDokument27 SeitenLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNoch keine Bewertungen
- CIRRHOSIS OF LIVER (Practice of Medicine)Dokument84 SeitenCIRRHOSIS OF LIVER (Practice of Medicine)simran kaurNoch keine Bewertungen
- Liver Cirrhosis: Review HepatologyDokument71 SeitenLiver Cirrhosis: Review HepatologyAstri Arri FebriantiNoch keine Bewertungen
- Approach To JaundiceDokument36 SeitenApproach To JaundiceNandita ChatterjeeNoch keine Bewertungen
- Liver CirrohosisDokument157 SeitenLiver CirrohosisSeema SachdevaNoch keine Bewertungen
- Hepatitis Acute Viral HepatitisDokument13 SeitenHepatitis Acute Viral HepatitisrhomaaanotesNoch keine Bewertungen
- 3 Liver Biliary TractDokument141 Seiten3 Liver Biliary Tractandreea0deyNoch keine Bewertungen
- Liver Cirrhosis and Its ComplicationsDokument34 SeitenLiver Cirrhosis and Its ComplicationsEthel ChakotaNoch keine Bewertungen
- JaundiceDokument17 SeitenJaundiceDarwithaNoch keine Bewertungen
- Liver Cirrhosis Causes, Symptoms & TreatmentDokument86 SeitenLiver Cirrhosis Causes, Symptoms & TreatmentKenMNoch keine Bewertungen
- Jaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TDokument35 SeitenJaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TSerge TresorNoch keine Bewertungen
- Acute Liver Disease: Causes and Types of Acute Hepatitis (38 charactersDokument22 SeitenAcute Liver Disease: Causes and Types of Acute Hepatitis (38 characterszakria100100Noch keine Bewertungen
- 3.liver & Biliary TractDokument141 Seiten3.liver & Biliary TractBobi WijayaNoch keine Bewertungen
- Liver & Biliary DiseaseDokument41 SeitenLiver & Biliary Diseasesaump3Noch keine Bewertungen
- Liver Pathology PDFDokument7 SeitenLiver Pathology PDFjohn smithNoch keine Bewertungen
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Dokument72 SeitenWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Darin MonerNoch keine Bewertungen
- Hepatobiliary System Note PDFDokument13 SeitenHepatobiliary System Note PDFMohd Syaiful Mohd ArisNoch keine Bewertungen
- Chapter 308Dokument10 SeitenChapter 308Lemuel LinoNoch keine Bewertungen
- CheungDokument104 SeitenCheungAndhita Satya Pratama GiovanniNoch keine Bewertungen
- HepatitisDokument24 SeitenHepatitisEric PeprahNoch keine Bewertungen
- Chronic Liver DiseasesDokument43 SeitenChronic Liver DiseasesDickson Luvi100% (1)
- Liver Cirrhosis LectureDokument83 SeitenLiver Cirrhosis LectureSheila Regina Tiza100% (1)
- Acute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetDokument40 SeitenAcute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetcoolcaesarNoch keine Bewertungen
- Question: 1 of 10 / Overall Score: 60%: True / FalseDokument11 SeitenQuestion: 1 of 10 / Overall Score: 60%: True / FalseGalaleldin AliNoch keine Bewertungen
- Liver Cirrhosis: Causes, Complications and ManagementDokument55 SeitenLiver Cirrhosis: Causes, Complications and ManagementAnonymous vUEDx8100% (1)
- 06 Interpretation of Diagnostics in The Case - KGDokument3 Seiten06 Interpretation of Diagnostics in The Case - KGGerarld Immanuel KairupanNoch keine Bewertungen
- Hepatic Disorders Guide for CliniciansDokument42 SeitenHepatic Disorders Guide for CliniciansMimmey Yeniw100% (1)
- 97Dokument79 Seiten97HATLERNoch keine Bewertungen
- LECTURES Liver PathophysiologyDokument118 SeitenLECTURES Liver PathophysiologyTarik100% (1)
- Pathology of LiverDokument15 SeitenPathology of Liverערין גבאריןNoch keine Bewertungen
- HepatitisDokument3 SeitenHepatitisRosendo Dacuyan100% (1)
- Liver CirrhosisDokument8 SeitenLiver CirrhosisDiana DeciuNoch keine Bewertungen
- Chronic Liver Disease and CirrhosisDokument5 SeitenChronic Liver Disease and Cirrhosisaqil ithninNoch keine Bewertungen
- 1-Discuss Hepatitis 2 - The Etio-Pathogenesis of Hepatitis 3 - Morphologic Features of Hepatitis - 4 - Clinical Features& Common ComplicationsDokument21 Seiten1-Discuss Hepatitis 2 - The Etio-Pathogenesis of Hepatitis 3 - Morphologic Features of Hepatitis - 4 - Clinical Features& Common ComplicationsANoch keine Bewertungen
- Hepatitis in Children: DR Hamza BawumiaDokument36 SeitenHepatitis in Children: DR Hamza BawumiaHamza BawumiaNoch keine Bewertungen
- Evaluation of Abnormal Liver Function Tests: DR Chris Hovell Consultant Gastroenterologist Dorset County HospitalDokument59 SeitenEvaluation of Abnormal Liver Function Tests: DR Chris Hovell Consultant Gastroenterologist Dorset County HospitalSaad MotawéaNoch keine Bewertungen
- Hepatitis Dan Sirosis HepatisDokument18 SeitenHepatitis Dan Sirosis HepatisIndri JayantiNoch keine Bewertungen
- Cirrhosis and Hepatocellular Carcinoma GuideDokument9 SeitenCirrhosis and Hepatocellular Carcinoma GuideGeorge WinchesterNoch keine Bewertungen
- Viral Hepatitis (Virus Hepatitis)Dokument60 SeitenViral Hepatitis (Virus Hepatitis)Ilmiah BagusNoch keine Bewertungen
- What? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanDokument45 SeitenWhat? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanM Rizky Assilmy LubisNoch keine Bewertungen
- Acute Hepatitis+alf 678Dokument37 SeitenAcute Hepatitis+alf 678Sheren GamaleldenNoch keine Bewertungen
- Cirrhosis: DR AkhondeiDokument111 SeitenCirrhosis: DR AkhondeiMuvenn KannanNoch keine Bewertungen
- 2 Approach To Elevated LFTDokument59 Seiten2 Approach To Elevated LFTparik2321Noch keine Bewertungen
- Covid 19 CPR 7 RulesDokument21 SeitenCovid 19 CPR 7 RulesMiguel Cuevas DolotNoch keine Bewertungen
- PSB 368Dokument6 SeitenPSB 368Miguel Cuevas DolotNoch keine Bewertungen
- Covid 19 CPR 7 RulesDokument21 SeitenCovid 19 CPR 7 RulesMiguel Cuevas DolotNoch keine Bewertungen
- Vertigo Gail Ishiyama 1 13 10Dokument40 SeitenVertigo Gail Ishiyama 1 13 10Myname Rama LienNoch keine Bewertungen
- Covid 19 PDFDokument18 SeitenCovid 19 PDFMiguel Cuevas DolotNoch keine Bewertungen
- Effectiveness of Transdermal MagnesiumDokument2 SeitenEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- How Can Patients Visitors Help - May18Dokument2 SeitenHow Can Patients Visitors Help - May18Miguel Cuevas DolotNoch keine Bewertungen
- Physical Examination in ENT: Ussana Promyothin, MDDokument60 SeitenPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNoch keine Bewertungen
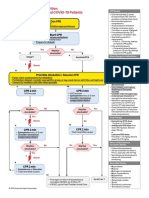
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDokument1 SeiteACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNoch keine Bewertungen
- (MED) COVID-19 Trans V. 2.0Dokument6 Seiten(MED) COVID-19 Trans V. 2.0Isabel VinasNoch keine Bewertungen
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Dokument30 SeitenClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNoch keine Bewertungen
- Physical Examination in ENT: Ussana Promyothin, MDDokument60 SeitenPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNoch keine Bewertungen
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDokument12 SeitenA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNoch keine Bewertungen
- Cook Book (Filipino) 13 PDFDokument23 SeitenCook Book (Filipino) 13 PDFAdina AnghelNoch keine Bewertungen
- Physical Assessment: Ear, Nose, Mouth, and ThroatDokument59 SeitenPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNoch keine Bewertungen
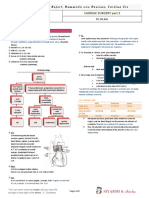
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDokument8 SeitenTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNoch keine Bewertungen
- Pedia Tickler Update 2017Dokument2 SeitenPedia Tickler Update 2017Tani BokNoch keine Bewertungen
- Benign Paroxysmal Positional Vertigo: Waseem WatadDokument37 SeitenBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNoch keine Bewertungen
- HEMAreviewDokument3 SeitenHEMAreviewMiguel Cuevas DolotNoch keine Bewertungen
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDokument12 SeitenA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNoch keine Bewertungen
- Nocturnals Physiology 2018Dokument14 SeitenNocturnals Physiology 2018Miguel Cuevas DolotNoch keine Bewertungen
- Active Listening HANDOUT PDFDokument26 SeitenActive Listening HANDOUT PDFMiguel Cuevas DolotNoch keine Bewertungen
- Clinical AbstractDokument4 SeitenClinical AbstractMiguel Cuevas DolotNoch keine Bewertungen
- Anesthesia Pocket Cards 7 18 18Dokument6 SeitenAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNoch keine Bewertungen
- Drug IndexDokument2 SeitenDrug IndexMiguel Cuevas DolotNoch keine Bewertungen
- Kerosene PDFDokument31 SeitenKerosene PDFRudyMLanaNoch keine Bewertungen
- Neurologic ExamDokument1 SeiteNeurologic ExamMiguel Cuevas DolotNoch keine Bewertungen
- Community-Acquired Pneumonia - CPG 2016Dokument26 SeitenCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNoch keine Bewertungen
- Pediatric History and Physical Exam GuideDokument7 SeitenPediatric History and Physical Exam GuideIndunil AnuruddhikaNoch keine Bewertungen
- 11-Immediate Care of NewbornDokument112 Seiten11-Immediate Care of NewbornJiela CarbonillaNoch keine Bewertungen
- Rubrics For Children in MurphyDokument18 SeitenRubrics For Children in MurphyVirag PatilNoch keine Bewertungen
- American Academy of Pediatrics: Term NewbornDokument10 SeitenAmerican Academy of Pediatrics: Term NewbornDaniel EspinozaNoch keine Bewertungen
- Neonatal Jaundice GuideDokument15 SeitenNeonatal Jaundice GuideSharan SekhonNoch keine Bewertungen
- Hemoglobin Catabolism and BilirubinDokument2 SeitenHemoglobin Catabolism and BilirubinJacob MasikaNoch keine Bewertungen
- Guideline HiperbilirubinemiaDokument20 SeitenGuideline HiperbilirubinemiaCaroline LimaNoch keine Bewertungen
- WHO Use of Anticoagulants and Stability of Samples PDFDokument64 SeitenWHO Use of Anticoagulants and Stability of Samples PDFImre DinnyesNoch keine Bewertungen
- Year 2: PBL 2: JaundiceDokument74 SeitenYear 2: PBL 2: JaundiceyaneemayNoch keine Bewertungen
- Hepatic Disorders Guide for CliniciansDokument42 SeitenHepatic Disorders Guide for CliniciansMimmey Yeniw100% (1)
- Fphar 08 00518Dokument22 SeitenFphar 08 00518Intan Princess SweetNoch keine Bewertungen
- CholilithiasisDokument94 SeitenCholilithiasisdr.hendraNoch keine Bewertungen
- Neonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoDokument46 SeitenNeonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoCarolyn CapisnonNoch keine Bewertungen
- Jaundice Newborn - 2Dokument15 SeitenJaundice Newborn - 2Miratunnisa AzzahrahNoch keine Bewertungen
- Speaking Sub-Test Overview: Roleplay StructureDokument23 SeitenSpeaking Sub-Test Overview: Roleplay Structureelite9491100% (2)
- Fatal Hepatitis from AcetazolamideDokument2 SeitenFatal Hepatitis from Acetazolamideمحمد فضل Fadhol RomdhoniNoch keine Bewertungen
- Lecture 1 - Introduc - On To Liver Cirrhosis and Liver Anatomy and PhysiologyDokument29 SeitenLecture 1 - Introduc - On To Liver Cirrhosis and Liver Anatomy and PhysiologyAmna HyderNoch keine Bewertungen
- JaundiceDokument3 SeitenJaundiceNyaoNyao MarcellanaNoch keine Bewertungen
- Digestive System: Yousef Ali Sazan Falah Snor Dilan KawtharDokument21 SeitenDigestive System: Yousef Ali Sazan Falah Snor Dilan Kawtharkauther hassanNoch keine Bewertungen
- Vitamin KDokument2 SeitenVitamin KDee Trooth100% (1)
- Chapter-09 - Examination of Digestive SystemDokument16 SeitenChapter-09 - Examination of Digestive SystemAnnahi BcNoch keine Bewertungen
- Pancreatic Cancer Early Detection, Diagnosis, and StagingDokument29 SeitenPancreatic Cancer Early Detection, Diagnosis, and StagingDokter LinggauNoch keine Bewertungen
- 480 MCQs With Answers of Goljan PathologyDokument382 Seiten480 MCQs With Answers of Goljan PathologySana Sheikh96% (28)
- Neonatal Jaundice: ObjectivesDokument12 SeitenNeonatal Jaundice: ObjectivesMadx VNoch keine Bewertungen
- Nbme 13Dokument10 SeitenNbme 13jettyvikasNoch keine Bewertungen
- Nursing Care Plan - HyperDokument4 SeitenNursing Care Plan - HyperJennalyn Casapao100% (1)
- Navodaya College of Nursing: Proforma For Registration of Subjects ForDokument18 SeitenNavodaya College of Nursing: Proforma For Registration of Subjects ForStephy SojanNoch keine Bewertungen
- Risk Factors Associated With Neonatal Jaundice: A Cross-Sectional Study From IranDokument7 SeitenRisk Factors Associated With Neonatal Jaundice: A Cross-Sectional Study From Iranariani khikmatul mazidahNoch keine Bewertungen
- A Bibliography of Medical Publications Relating To Sri Lanka, 1811 - 1976Dokument443 SeitenA Bibliography of Medical Publications Relating To Sri Lanka, 1811 - 1976Fiona Kumari CampbellNoch keine Bewertungen
- Appearance of The Baby-Resource UnitDokument15 SeitenAppearance of The Baby-Resource UnitLucañas PringelNoch keine Bewertungen
- NCK Examination Past Pps1,2,3,4-1Dokument59 SeitenNCK Examination Past Pps1,2,3,4-1jimwao100% (1)