Das könnte Ihnen auch gefallen
- Pressure UlcerDokument126 SeitenPressure UlcerSyabie Yassin100% (1)
- Pathfinder BloodforgeDokument98 SeitenPathfinder BloodforgeLK100% (11)
- Shoulder Biomechanics: Roberto Lugo, Peter Kung, C. Benjamin MaDokument11 SeitenShoulder Biomechanics: Roberto Lugo, Peter Kung, C. Benjamin MaAbyudya Rafif KurniawanNoch keine Bewertungen
- (New Procedures in Spinal Interventional Neuroradiology) Luigi Manfrà (Eds.) - Spinal Canal Stenosis-Springer International PublisDokument98 Seiten(New Procedures in Spinal Interventional Neuroradiology) Luigi Manfrà (Eds.) - Spinal Canal Stenosis-Springer International PublisThuyet Nguyen PhuocNoch keine Bewertungen
- Dengue Expanded Syndromes 4Dokument167 SeitenDengue Expanded Syndromes 4drhwek2001Noch keine Bewertungen
- Lesson Plan Human Reproductive SystemDokument2 SeitenLesson Plan Human Reproductive SystemGarnis HakimNoch keine Bewertungen
- Thomas J. Fogarty MD, Amitava Biswas MD (Auth.), Thomas J. Fogarty, Rodney A. White (Eds.) - Peripheral Endovascular Interventions-Springer-Verlag New York (2010)Dokument509 SeitenThomas J. Fogarty MD, Amitava Biswas MD (Auth.), Thomas J. Fogarty, Rodney A. White (Eds.) - Peripheral Endovascular Interventions-Springer-Verlag New York (2010)Mircea Eugen MutuNoch keine Bewertungen
- Chest Trauma and SurgeryDokument67 SeitenChest Trauma and SurgeryKapil LakhwaraNoch keine Bewertungen
- Initial Assessment AND ManagementDokument30 SeitenInitial Assessment AND ManagementSikaNoch keine Bewertungen
- Wound Care Giudeline NHS Bolton HospitalDokument44 SeitenWound Care Giudeline NHS Bolton HospitalJumatun Mona WarahNoch keine Bewertungen
- Clinical Practice Guidelines 2012Dokument50 SeitenClinical Practice Guidelines 2012Immanuel Van Donn Batubara100% (1)
- PICU HandbookDokument113 SeitenPICU HandbookEdu WilliamNoch keine Bewertungen
- Endometrial Malignancies 1Dokument41 SeitenEndometrial Malignancies 1jerrydanfordfxNoch keine Bewertungen
- PediatricsDokument79 SeitenPediatricsapi-3712326Noch keine Bewertungen
- Initial Assessment and ManagementDokument8 SeitenInitial Assessment and ManagementAlvin De LunaNoch keine Bewertungen
- Play in Child Development andDokument194 SeitenPlay in Child Development andAlinaZbarloiu100% (4)
- CroupDokument13 SeitenCroupEdu William100% (1)
- Management of Multiple Traumatised PatientDokument4 SeitenManagement of Multiple Traumatised PatientOmar MohammedNoch keine Bewertungen
- ABCs of Thoracic TraumaDokument5 SeitenABCs of Thoracic TraumaAlice S ChangNoch keine Bewertungen
- Trauma OverviewDokument48 SeitenTrauma OverviewFrancescoBarbero100% (1)
- Queensland Health Falls Best Practice Guide - 1 PDFDokument117 SeitenQueensland Health Falls Best Practice Guide - 1 PDFshobaNoch keine Bewertungen
- Diagnosis and Treatment of Intraabdominal InjuriesDokument88 SeitenDiagnosis and Treatment of Intraabdominal Injuriessgod34Noch keine Bewertungen
- Operation NotesDokument7 SeitenOperation NotessduxNoch keine Bewertungen
- Neurological ExaminationDokument8 SeitenNeurological Examinationg8048658Noch keine Bewertungen
- Revisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesDokument8 SeitenRevisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesTiti Multi SaariNoch keine Bewertungen
- Atlas of Airway Management - Techniques and Tools (PDFDrive)Dokument433 SeitenAtlas of Airway Management - Techniques and Tools (PDFDrive)Yanuar AbdulhayNoch keine Bewertungen
- Skin Integrity and Wound CareDokument47 SeitenSkin Integrity and Wound CareCHALIE MEQUNoch keine Bewertungen
- Slides For Hand Hygiene CoordinatorDokument138 SeitenSlides For Hand Hygiene CoordinatorPaola Alcal� MatusNoch keine Bewertungen
- Life Vision Upper Intermediate WorkbookDokument129 SeitenLife Vision Upper Intermediate WorkbookGrace FreudNoch keine Bewertungen
- Approach To BreathlessnessDokument5 SeitenApproach To BreathlessnessEdy GunawanNoch keine Bewertungen
- W1L1 - Initial Assessment For Trauma - 2Dokument44 SeitenW1L1 - Initial Assessment For Trauma - 2Baihaqi SaharunNoch keine Bewertungen
- Early Warning Score & Rapid Response TeamDokument26 SeitenEarly Warning Score & Rapid Response TeamAsim IdreesNoch keine Bewertungen
- Pediatric Vascular Neurosurgery (Part 2)Dokument263 SeitenPediatric Vascular Neurosurgery (Part 2)lailaakely.fisioNoch keine Bewertungen
- Infectious Diseases in Pediatric Otolaryngology A Practical Guide by Tulio A. Valdez, Jesus G. VallejoDokument242 SeitenInfectious Diseases in Pediatric Otolaryngology A Practical Guide by Tulio A. Valdez, Jesus G. VallejoNguyễn ThànhNoch keine Bewertungen
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDokument13 Seiten00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNoch keine Bewertungen
- Pediatric Urology: Surgical Complications and ManagementVon EverandPediatric Urology: Surgical Complications and ManagementNoch keine Bewertungen
- 10 Patient Safety and Invasive ProceduresDokument4 Seiten10 Patient Safety and Invasive Proceduresanojan100% (1)
- Pedtext 5Dokument716 SeitenPedtext 5jay_eshwa100% (1)
- Best ICU Cases2022Dokument618 SeitenBest ICU Cases2022sumanth aryaNoch keine Bewertungen
- Evaluation of Dyspneic PatientDokument15 SeitenEvaluation of Dyspneic Patientcamila perillaNoch keine Bewertungen
- Physiology Question Bank FinalDokument16 SeitenPhysiology Question Bank Finalatefmabood100% (2)
- Pediatric Umbilical Reconstruction Principles and Techniques by Shiffman, Melvin ADokument185 SeitenPediatric Umbilical Reconstruction Principles and Techniques by Shiffman, Melvin AСергей АбрамовNoch keine Bewertungen
- Anesthesia and Perioperative Care For Organ Transplantation-Kathirvel Subramaniam, Tetsuro Sakai (Eds.) - ASpringer-Verlag New York (2017) - Repaired PDFDokument572 SeitenAnesthesia and Perioperative Care For Organ Transplantation-Kathirvel Subramaniam, Tetsuro Sakai (Eds.) - ASpringer-Verlag New York (2017) - Repaired PDFmarcoNoch keine Bewertungen
- Lunch Symposium Dr. Fanny Indarto, SPB - Multiple vs. Mass Casualties ManagementDokument17 SeitenLunch Symposium Dr. Fanny Indarto, SPB - Multiple vs. Mass Casualties ManagementThomas Kwee100% (1)
- Essential Tissue Healing of the Face and NeckVon EverandEssential Tissue Healing of the Face and NeckBewertung: 5 von 5 Sternen5/5 (2)
- JWC Convatec Wound-Hygiene-28pp 14-Feb CA Web-LicDokument28 SeitenJWC Convatec Wound-Hygiene-28pp 14-Feb CA Web-LicAjeng Kania100% (1)
- Meatotomy and Wound CareDokument13 SeitenMeatotomy and Wound CareAgung IndraNoch keine Bewertungen
- Fundamentals of Surgical 3rd EdDokument9 SeitenFundamentals of Surgical 3rd EdRahmania Mutia RifaniNoch keine Bewertungen
- McGoldrick - Infection Control Ritual To Science - Based PracticeDokument8 SeitenMcGoldrick - Infection Control Ritual To Science - Based PracticeUswaPutriemelelaNoch keine Bewertungen
- Advances in Emergent Airway Management in PediatricsDokument19 SeitenAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNoch keine Bewertungen
- British Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyDokument6 SeitenBritish Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyPriscilla CarmiolNoch keine Bewertungen
- Modern Wound Care - Lohmann & RauscherDokument18 SeitenModern Wound Care - Lohmann & Rauschersins1984Noch keine Bewertungen
- Emergency Department Patient KioskDokument11 SeitenEmergency Department Patient Kioskapi-488097590Noch keine Bewertungen
- Manejo de Las Crisis en Anestesia - Gaba 2 Ed PDFDokument424 SeitenManejo de Las Crisis en Anestesia - Gaba 2 Ed PDFdianisssuxNoch keine Bewertungen
- ABCs of Wound DebridementDokument3 SeitenABCs of Wound DebridementSheril MarekNoch keine Bewertungen
- Recruitment Maneuvers and PEEP TitrationDokument17 SeitenRecruitment Maneuvers and PEEP TitrationDiego Cruces OrdoñezNoch keine Bewertungen
- Acute Viral Gastroenteritis in Children in Resource-Rich Countries - Clinical Features and DiagnosisDokument19 SeitenAcute Viral Gastroenteritis in Children in Resource-Rich Countries - Clinical Features and DiagnosisNuno AlmeidaNoch keine Bewertungen
- Approach To Septic ShockDokument16 SeitenApproach To Septic ShockRaja EllysyaNoch keine Bewertungen
- Wound CareDokument11 SeitenWound Carenichole9981Noch keine Bewertungen
- Central Line Removal ProtocolDokument1 SeiteCentral Line Removal Protocolmathurarun2000Noch keine Bewertungen
- Abdominal Pain in PaediatricDokument35 SeitenAbdominal Pain in PaediatricNuyue FathihahNoch keine Bewertungen
- Infection Control in NICUDokument9 SeitenInfection Control in NICUMike CalipayanNoch keine Bewertungen
- ABC of Wound Healing PDFDokument4 SeitenABC of Wound Healing PDFMrJPhaetonNoch keine Bewertungen
- Atls 1Dokument5 SeitenAtls 1Mega MalyndaNoch keine Bewertungen
- Neurologic Assessment RationaleDokument16 SeitenNeurologic Assessment RationaleflorenzoNoch keine Bewertungen
- Obstetric HDU and ICU: Guidelines ForDokument52 SeitenObstetric HDU and ICU: Guidelines ForsidharthNoch keine Bewertungen
- Handbook Peads SurgDokument88 SeitenHandbook Peads Surgsedaka26Noch keine Bewertungen
- Thoracic Surgery Secrets Book PDFDokument4 SeitenThoracic Surgery Secrets Book PDFRishi MangalNoch keine Bewertungen
- Classification of Medical ProceduresDokument1.401 SeitenClassification of Medical Proceduresthe_albenaNoch keine Bewertungen
- Disaster NursingDokument51 SeitenDisaster NursingEdra VillanuevaNoch keine Bewertungen
- Perioperative Scope of ServicesDokument2 SeitenPerioperative Scope of Servicesmonir61Noch keine Bewertungen
- 2000 Trauma ManagementDokument691 Seiten2000 Trauma ManagementSon Nguyen100% (4)
- Kjeldsberg Chap 1Dokument14 SeitenKjeldsberg Chap 1Joyee BasuNoch keine Bewertungen
- Laser Guidance Notes 101212Dokument3 SeitenLaser Guidance Notes 101212Edu WilliamNoch keine Bewertungen
- Dietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Dokument1 SeiteDietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Edu WilliamNoch keine Bewertungen
- Modified Finnegan ScoringDokument4 SeitenModified Finnegan ScoringEdu WilliamNoch keine Bewertungen
- Pediatric Advanced Life Support Provider Manual: January 2012Dokument1 SeitePediatric Advanced Life Support Provider Manual: January 2012Danhil RamosNoch keine Bewertungen
- Fast Food For Our Preemies .3Dokument2 SeitenFast Food For Our Preemies .3Edu WilliamNoch keine Bewertungen
- Pressure Ulcer Assessment CardDokument2 SeitenPressure Ulcer Assessment CardEdu WilliamNoch keine Bewertungen
- General PediatricsDokument36 SeitenGeneral PediatricsEdu WilliamNoch keine Bewertungen
- Adolescent Medicine IDokument45 SeitenAdolescent Medicine Iapi-3712326100% (1)
- Membaca EkgDokument90 SeitenMembaca EkgEdu WilliamNoch keine Bewertungen
- Amnioinfusion For The Prevention of MASDokument9 SeitenAmnioinfusion For The Prevention of MASEdu WilliamNoch keine Bewertungen
- Body Size in DHFDokument6 SeitenBody Size in DHFEdu WilliamNoch keine Bewertungen
- Advanced Management of MASDokument7 SeitenAdvanced Management of MASEdu WilliamNoch keine Bewertungen
- 12 - Asthma PDFDokument21 Seiten12 - Asthma PDFjuniorebindaNoch keine Bewertungen
- Tanner MethodDokument8 SeitenTanner MethodEdu WilliamNoch keine Bewertungen
- Asthma v.3.0: Criteria and Respiratory ScoreDokument36 SeitenAsthma v.3.0: Criteria and Respiratory ScoreYudha Astipamara PanjayaNoch keine Bewertungen
- Pediatric Surgery HandbookDokument29 SeitenPediatric Surgery HandbookEdu WilliamNoch keine Bewertungen
- Pert PDFDokument18 SeitenPert PDFKhalilah AisyahNoch keine Bewertungen
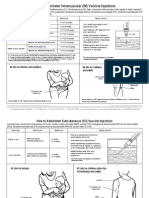
- How To Admister VaccineDokument2 SeitenHow To Admister VaccineEdu WilliamNoch keine Bewertungen
- Field Guide: Surveillance of Acute Flaccid ParalysisDokument49 SeitenField Guide: Surveillance of Acute Flaccid ParalysissmopunhnanaNoch keine Bewertungen
- MMRVDokument2 SeitenMMRVMichael HalimNoch keine Bewertungen
- Japanese Encephalitis - 2011Dokument2 SeitenJapanese Encephalitis - 2011Edu WilliamNoch keine Bewertungen
- HPV (Gardasil) - 2011Dokument2 SeitenHPV (Gardasil) - 2011Edu WilliamNoch keine Bewertungen
- Genu Varum & Genu Valgum in Children: Written by August 10, 2020Dokument3 SeitenGenu Varum & Genu Valgum in Children: Written by August 10, 2020haide786Noch keine Bewertungen
- Article Review Kel 3 KompilasiDokument21 SeitenArticle Review Kel 3 KompilasiFazlin KhuzaimaNoch keine Bewertungen
- 2010 Spinner Air-Suspension Fork ManualDokument8 Seiten2010 Spinner Air-Suspension Fork Manualxpert_vt100% (1)
- Ovo Kao Nebi Trebalo PostojatiDokument2 SeitenOvo Kao Nebi Trebalo PostojatiBoris KrizmanicNoch keine Bewertungen
- Pathfit 1 M3Dokument20 SeitenPathfit 1 M3rainiel gibasNoch keine Bewertungen
- 08-12-2019 (20.30), Ch. Ivan, 14 Yo, Close Fraktur 1-3 Distal Os Radius Dextra, Dr. Tri Tuty H, SP - OtDokument14 Seiten08-12-2019 (20.30), Ch. Ivan, 14 Yo, Close Fraktur 1-3 Distal Os Radius Dextra, Dr. Tri Tuty H, SP - OtRa' DesireeNoch keine Bewertungen
- Lazy Girl WorkoutDokument17 SeitenLazy Girl Workoutسميره محمدNoch keine Bewertungen
- Tool Operating Manual Tool Operating Manual: 276-7273 Cylinder Sensor Test Box (In Cylinder Function Test)Dokument12 SeitenTool Operating Manual Tool Operating Manual: 276-7273 Cylinder Sensor Test Box (In Cylinder Function Test)CarlosNoch keine Bewertungen
- Hand Assessment - 3rd YrDokument54 SeitenHand Assessment - 3rd YrSURBHI AGRAWALNoch keine Bewertungen
- Hip, Knee, Ankle PROMDokument28 SeitenHip, Knee, Ankle PROMsxsparsh2305Noch keine Bewertungen
- Prelim Paper 1 GMERS GandhinagarDokument2 SeitenPrelim Paper 1 GMERS GandhinagarcontacbymeNoch keine Bewertungen
- Lower-Nerve FlossingDokument1 SeiteLower-Nerve Flossingdobrica ilicNoch keine Bewertungen
- Rodney ColleyDokument30 SeitenRodney Colleyefuchs160100% (1)
- Catapang - People Vs DioDokument3 SeitenCatapang - People Vs DioDorothy Joy LucmayonNoch keine Bewertungen
- People v. Clarence Lee Scott, Court of Appeals of California, Fifth District. Opinion (3/3/11)Dokument8 SeitenPeople v. Clarence Lee Scott, Court of Appeals of California, Fifth District. Opinion (3/3/11)Peter M. HeimlichNoch keine Bewertungen
- Fuji Portaflow Instruction ManualDokument194 SeitenFuji Portaflow Instruction Manualgreggles69Noch keine Bewertungen
- The Scapula - Surfaces - Fractures - Winging - TeachMeAnatomyDokument3 SeitenThe Scapula - Surfaces - Fractures - Winging - TeachMeAnatomyDelta MuNoch keine Bewertungen
- Date/Schedule Activities Expected Output Verified/Checked by Area in ChargeDokument2 SeitenDate/Schedule Activities Expected Output Verified/Checked by Area in ChargeJobelle AcenaNoch keine Bewertungen
- History and Assessment & Anatomy and Physiology of BurnsDokument10 SeitenHistory and Assessment & Anatomy and Physiology of BurnsRina MaeNoch keine Bewertungen
- Service Station Emergency PlanDokument20 SeitenService Station Emergency PlanScribdTranslationsNoch keine Bewertungen
- Presented By:-Dr. Sushma Tomar Associate Professor Department of AnatomyDokument20 SeitenPresented By:-Dr. Sushma Tomar Associate Professor Department of AnatomyCristine EchaveNoch keine Bewertungen
- Slipped Capital Femoral Epiphysis - SCFEDokument3 SeitenSlipped Capital Femoral Epiphysis - SCFEyosua_edwin100% (1)