Das könnte Ihnen auch gefallen
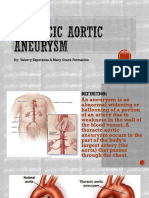
- Thoracic Aortic AneurysmDokument17 SeitenThoracic Aortic AneurysmGlyssa CabarrubiasNoch keine Bewertungen
- AtherosclerosisDokument6 SeitenAtherosclerosisNader Smadi100% (1)
- Cardiogenic ShockDokument20 SeitenCardiogenic Shockanimesh pandaNoch keine Bewertungen
- Pathology of Cardiovascular SystemDokument75 SeitenPathology of Cardiovascular Systemefri100% (2)
- Polygenic and Multifactorial Diseases: - Key Features and Isolation of Responsible Genes Newcastle 13th December 2007Dokument34 SeitenPolygenic and Multifactorial Diseases: - Key Features and Isolation of Responsible Genes Newcastle 13th December 2007Fidia FibrianaNoch keine Bewertungen
- Pathophysiology of AtherosclerosisDokument27 SeitenPathophysiology of AtherosclerosisAmira Paguyo QuilapioNoch keine Bewertungen
- SpermatogenesisDokument24 SeitenSpermatogenesisOmm KoliNoch keine Bewertungen
- Congestive Heart FailureDokument25 SeitenCongestive Heart FailuredevianiamalinaNoch keine Bewertungen
- Hemorrhagic Cerebro Vascular DiseaseDokument37 SeitenHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Cardiac TamponadeDokument10 SeitenCardiac TamponadeRahmi Fatma SariNoch keine Bewertungen
- Development of The Cardiovascular SystemDokument9 SeitenDevelopment of The Cardiovascular SystemKeshant SamarooNoch keine Bewertungen
- Myocardial InfarctionDokument23 SeitenMyocardial InfarctionNishaThakuri100% (1)
- Cerebrovascular Accident (CVA)Dokument71 SeitenCerebrovascular Accident (CVA)nur muizzah afifah hussinNoch keine Bewertungen
- Legal MedDokument2 SeitenLegal MedHanna Supetran0% (1)
- Class Presentation ON Acute Tubular NecrosisDokument39 SeitenClass Presentation ON Acute Tubular NecrosisDeeksha RajputNoch keine Bewertungen
- Cerebrovascular AccidentDokument8 SeitenCerebrovascular Accidentplethoraldork100% (10)
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDokument4 SeitenPathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiNoch keine Bewertungen
- Anatomy and Physiology of Blood VesselDokument3 SeitenAnatomy and Physiology of Blood Vesselneleh grayNoch keine Bewertungen
- Anatomy Myocardial InfarctionDokument5 SeitenAnatomy Myocardial InfarctionLyka Milo AvilaNoch keine Bewertungen
- Ischemic Heart Disease PWDokument13 SeitenIschemic Heart Disease PWEunica RamosNoch keine Bewertungen
- Myocardial Infarction: Practice Essentials, Background, Definitions PDFDokument12 SeitenMyocardial Infarction: Practice Essentials, Background, Definitions PDFMukhtar UllahNoch keine Bewertungen
- Mike Adams - The Healing Power of Sunlight Vitamin DDokument26 SeitenMike Adams - The Healing Power of Sunlight Vitamin DJOSEPHNoch keine Bewertungen
- Cardiac TamponadeDokument3 SeitenCardiac TamponadeKimberly SolisNoch keine Bewertungen
- Autoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinDokument8 SeitenAutoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinFedoxyzNoch keine Bewertungen
- Cardiogenic ShockDokument21 SeitenCardiogenic ShockIslamOteshNoch keine Bewertungen
- Rheumatic FeverDokument3 SeitenRheumatic FeverKhalid Mahmud Arifin100% (3)
- Pleural EffusionDokument4 SeitenPleural Effusionrezairfan221Noch keine Bewertungen
- Gender DysphoriaDokument5 SeitenGender DysphoriaJavedNoch keine Bewertungen
- Hemodynamic Disorders, Thromboembolic DiseasesDokument100 SeitenHemodynamic Disorders, Thromboembolic DiseasesKate Alyssa Caton100% (1)
- NeisseriaDokument32 SeitenNeisseriaKeshant SamarooNoch keine Bewertungen
- 9 ThrombosisDokument18 Seiten9 ThrombosisEslam Almassri100% (1)
- Atherosclerosis 2 2017 (Modified)Dokument64 SeitenAtherosclerosis 2 2017 (Modified)Remo B AbyNoch keine Bewertungen
- Movement DisordersDokument10 SeitenMovement DisordersAli 10Noch keine Bewertungen
- Atheroma: 2 History of ResearchDokument7 SeitenAtheroma: 2 History of ResearchZiedTrikiNoch keine Bewertungen
- Pathophysiology of Heart FailureDokument4 SeitenPathophysiology of Heart FailureTiger Knee100% (2)
- Stroke and Cerebrovascular DiseaseDokument14 SeitenStroke and Cerebrovascular DiseaseMarwan M.Noch keine Bewertungen
- NCBI ResourcesDokument13 SeitenNCBI ResourceshamzaloNoch keine Bewertungen
- Congestive Heart FailureDokument19 SeitenCongestive Heart FailureIlavenil PanduranganNoch keine Bewertungen
- Infective EndocarditisDokument68 SeitenInfective EndocarditisDr. Rajesh PadhiNoch keine Bewertungen
- Pa Tho Physiology of Hemorrhagic StrokeDokument2 SeitenPa Tho Physiology of Hemorrhagic StrokeMerlash MerlaNoch keine Bewertungen
- Atherosclerosis and ArteriosclerosisDokument50 SeitenAtherosclerosis and ArteriosclerosisApril Carter100% (1)
- Acute Myocardial InfarctionDokument20 SeitenAcute Myocardial InfarctionDavid Christian CalmaNoch keine Bewertungen
- Myocardial InfarctionDokument15 SeitenMyocardial InfarctionameerNoch keine Bewertungen
- Coronary Artery DiseaseDokument80 SeitenCoronary Artery Diseaseamelia pratiwiNoch keine Bewertungen
- Aneurysm PDFDokument20 SeitenAneurysm PDFKV100% (1)
- 403 Full PDFDokument10 Seiten403 Full PDFKuroto YoshikiNoch keine Bewertungen
- Concept Map AAADokument6 SeitenConcept Map AAASandrine BarredoNoch keine Bewertungen
- Intestinal ObstructionDokument27 SeitenIntestinal ObstructionAna AvilaNoch keine Bewertungen
- DB13 - Pathophysiology of AtherosclerosisDokument2 SeitenDB13 - Pathophysiology of Atherosclerosisi_vhie03Noch keine Bewertungen
- Hepatomegaly 1Dokument5 SeitenHepatomegaly 1Bobby ParksNoch keine Bewertungen
- Ischemic StrokeDokument7 SeitenIschemic StrokeAlly Juaneza100% (1)
- Renal DisordersDokument77 SeitenRenal Disorderslorelee_espaldon100% (1)
- Left Heart FailureDokument2 SeitenLeft Heart FailureJechelle Ann Pabustan Martin-Boniquit100% (1)
- CHF PathophysiologyDokument4 SeitenCHF PathophysiologyVirtudazo JessaNoch keine Bewertungen
- MIDokument22 SeitenMIGagauz SiliviaNoch keine Bewertungen
- PericarditisDokument3 SeitenPericarditisKhalid Mahmud Arifin0% (1)
- Human Diseases Case Study 18 ADokument4 SeitenHuman Diseases Case Study 18 Aairickann100% (1)
- Infective EndocarditisDokument66 SeitenInfective Endocarditissanjivdas100% (4)
- Congestive Heart Failure OverviewDokument12 SeitenCongestive Heart Failure OverviewkazelleNoch keine Bewertungen
- Acute Myocardial InfarctionDokument2 SeitenAcute Myocardial InfarctionhailleyannNoch keine Bewertungen
- Complication of Blood TransfusionDokument5 SeitenComplication of Blood TransfusionChey Ochy ApriliaNoch keine Bewertungen
- ArteriosclerosisDokument8 SeitenArteriosclerosisDr. Bushra SumraNoch keine Bewertungen
- Role of The Kidney in Long Term RegulationDokument19 SeitenRole of The Kidney in Long Term RegulationMelisa NovitasariNoch keine Bewertungen
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDokument5 SeitenDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNoch keine Bewertungen
- Anemia IntroductionDokument15 SeitenAnemia IntroductionNitesh Kotian100% (1)
- Anaphylactic ShockDokument19 SeitenAnaphylactic ShockrutiranNoch keine Bewertungen
- Bladder CancerDokument35 SeitenBladder CancerHealth Education Library for PeopleNoch keine Bewertungen
- ThrombosisDokument27 SeitenThrombosischaritykimberly3Noch keine Bewertungen
- 6 ThrombosisDokument27 Seiten6 ThrombosisBravan AliennNoch keine Bewertungen
- 2002Dokument10 Seiten2002Keshant SamarooNoch keine Bewertungen
- Resit SAQ 2016Dokument10 SeitenResit SAQ 2016Keshant SamarooNoch keine Bewertungen
- StrepDokument72 SeitenStrepKeshant SamarooNoch keine Bewertungen
- 2012 Final Year Exam - General SurgeryDokument3 Seiten2012 Final Year Exam - General SurgeryKeshant SamarooNoch keine Bewertungen
- 18 - Neonatal SZDokument41 Seiten18 - Neonatal SZKeshant SamarooNoch keine Bewertungen
- 2011 Surgery Short AnswerDokument1 Seite2011 Surgery Short AnswerKeshant SamarooNoch keine Bewertungen
- 1 Staphylococcus Lecture 1 Last YearDokument39 Seiten1 Staphylococcus Lecture 1 Last YearKeshant Samaroo100% (1)
- Story of A Broken TeenDokument1 SeiteStory of A Broken TeenKeshant SamarooNoch keine Bewertungen
- Potassium: Keshant SamarooDokument14 SeitenPotassium: Keshant SamarooKeshant SamarooNoch keine Bewertungen
- Story of A Broken ChildDokument1 SeiteStory of A Broken ChildKeshant SamarooNoch keine Bewertungen
- Story of A Broken TeenDokument1 SeiteStory of A Broken TeenKeshant SamarooNoch keine Bewertungen
- Signs and SymptomsDokument3 SeitenSigns and SymptomsKeshant SamarooNoch keine Bewertungen
- Ischemic Heart Disease, Myocardial Infarction and Hypertensive Heart DiseaseDokument4 SeitenIschemic Heart Disease, Myocardial Infarction and Hypertensive Heart DiseaseKeshant SamarooNoch keine Bewertungen
- Disease of Blood VesselsDokument5 SeitenDisease of Blood VesselsKeshant SamarooNoch keine Bewertungen
- Forensic Medicine & Toxicology: Trace Evidences - Semen, Saliva, Hair & FibersDokument31 SeitenForensic Medicine & Toxicology: Trace Evidences - Semen, Saliva, Hair & FibersKeshant SamarooNoch keine Bewertungen
- Forensic Medicine & Toxicology: Trace Evidences - Semen, Saliva, Hair & FibersDokument31 SeitenForensic Medicine & Toxicology: Trace Evidences - Semen, Saliva, Hair & FibersKeshant SamarooNoch keine Bewertungen
- Clinical CourseDokument3 SeitenClinical CourseKeshant SamarooNoch keine Bewertungen
- Thorax 1 WallDokument9 SeitenThorax 1 WallKeshant SamarooNoch keine Bewertungen
- Medical Practioner's Act 1998 Ch3202Dokument24 SeitenMedical Practioner's Act 1998 Ch3202Keshant SamarooNoch keine Bewertungen
- Cfa DraftDokument27 SeitenCfa DraftKeshant SamarooNoch keine Bewertungen
- Fetal Alcohol SyndromeDokument2 SeitenFetal Alcohol SyndromeKeshant SamarooNoch keine Bewertungen
- East Indian Perception of HIVDokument2 SeitenEast Indian Perception of HIVKeshant SamarooNoch keine Bewertungen
- Law CIE 2014-SyllabusDokument23 SeitenLaw CIE 2014-SyllabusKeshant SamarooNoch keine Bewertungen
- Introduction To ANSDokument40 SeitenIntroduction To ANSKeshant SamarooNoch keine Bewertungen
- Chapter 76:: Vitiligo:: Khaled Ezzedine & John E. HarrisDokument17 SeitenChapter 76:: Vitiligo:: Khaled Ezzedine & John E. HarrisHellenPertiwiWulandariNoch keine Bewertungen
- Transfer Rnas As Dynamic and Critical Regulators of Cancer ProgressionDokument16 SeitenTransfer Rnas As Dynamic and Critical Regulators of Cancer Progressionliliana-contrerasNoch keine Bewertungen
- Complex Patterns of Inheritance NotebookDokument4 SeitenComplex Patterns of Inheritance NotebookFarah abu hashimNoch keine Bewertungen
- Org - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFDokument2 SeitenOrg - Telegram.messenger - Provider Media Telegram Telegram Documents 4 5985610863455765491 PDFsameeNoch keine Bewertungen
- Draft Guidelines Housing MiceDokument136 SeitenDraft Guidelines Housing MiceindrieliciousNoch keine Bewertungen
- Aklimatisasi Hewan CobaDokument6 SeitenAklimatisasi Hewan CobaNurma FitriaNoch keine Bewertungen
- Subtractive Genomic HybridizationDokument12 SeitenSubtractive Genomic HybridizationRatan RatanNoch keine Bewertungen
- Review: Lenat Joffe, Elena J LadasDokument11 SeitenReview: Lenat Joffe, Elena J LadasGUSTAVO BELLONoch keine Bewertungen
- Genome Data Mining: One Linkage Score Per DNA Letter.Dokument16 SeitenGenome Data Mining: One Linkage Score Per DNA Letter.Korkut VataNoch keine Bewertungen
- Journal Issaas v15n1 POSTER ABSTRACTSDokument28 SeitenJournal Issaas v15n1 POSTER ABSTRACTSChai YawatNoch keine Bewertungen
- Article Type: Original ArticleDokument30 SeitenArticle Type: Original ArticlemeizanNoch keine Bewertungen
- Moringa OleiferaDokument4 SeitenMoringa Oleiferajap pagharionNoch keine Bewertungen
- Lactose Intolerance Pada AnakDokument11 SeitenLactose Intolerance Pada AnakWilliam MakdinataNoch keine Bewertungen
- Oncogene: Viral OncogenesDokument12 SeitenOncogene: Viral OncogenesIlyas Khan AurakzaiNoch keine Bewertungen
- A 3. Pengenalan VirusDokument18 SeitenA 3. Pengenalan VirusQhus YairyNoch keine Bewertungen
- Ariffuddin, Fatima-Nangco L. BSBA O.M IDokument7 SeitenAriffuddin, Fatima-Nangco L. BSBA O.M Ikimea03Noch keine Bewertungen
- Biology Syllabus HSEBDokument2 SeitenBiology Syllabus HSEBDipesh ShresthaNoch keine Bewertungen
- Pohon Masalah AnsietasDokument16 SeitenPohon Masalah AnsietasDeva NatarummandaNoch keine Bewertungen
- Thyroid Pathophysiology and Diagnostic Evaluation: Chapter OutlineDokument38 SeitenThyroid Pathophysiology and Diagnostic Evaluation: Chapter OutlinePedro Gómez RNoch keine Bewertungen
- Akt RenalDokument4 SeitenAkt Renaldzidek7Noch keine Bewertungen
- HemoglobinDokument15 SeitenHemoglobinArya RaoNoch keine Bewertungen
- Make A Short DNA ModelDokument5 SeitenMake A Short DNA ModelShashank TiwariNoch keine Bewertungen