Das könnte Ihnen auch gefallen
- Post Term PregnancyDokument35 SeitenPost Term PregnancyNishaThakuri100% (2)
- Maternal NewbornDokument2 SeitenMaternal NewborntmanareNoch keine Bewertungen
- Ncma219 - 3Dokument2 SeitenNcma219 - 3IRA ODETTE GATUSNoch keine Bewertungen
- Antepartum AssessmentDokument14 SeitenAntepartum Assessmentamena mahmoudNoch keine Bewertungen
- Antepartum Fetal Assessment 2018Dokument39 SeitenAntepartum Fetal Assessment 2018amena mahmoudNoch keine Bewertungen
- 6 Antepartum Care PDFDokument24 Seiten6 Antepartum Care PDFmohammed farajiNoch keine Bewertungen
- Obstetric Operations & Procedures2Dokument98 SeitenObstetric Operations & Procedures2mohazemalhotraNoch keine Bewertungen
- Factors to Consider Before Labor Augmentation with OxytocinDokument3 SeitenFactors to Consider Before Labor Augmentation with OxytocinCelynn BalingitNoch keine Bewertungen
- Prenatal Care Objectives & Antepartum AssessmentDokument7 SeitenPrenatal Care Objectives & Antepartum AssessmentRyubusa HayabusaNoch keine Bewertungen
- Assessment of The Fetal Well-BeingDokument85 SeitenAssessment of The Fetal Well-BeingAlphine DalgoNoch keine Bewertungen
- Asphyxia BrieferDokument4 SeitenAsphyxia BrieferNewborn2013Noch keine Bewertungen
- Stages of Labor NSG MGTDokument3 SeitenStages of Labor NSG MGTMelDred Cajes BolandoNoch keine Bewertungen
- MCQ - On Obstetrics and Gynaecology PART 2Dokument78 SeitenMCQ - On Obstetrics and Gynaecology PART 2Kripa Susan100% (3)
- Written Report Prenatal Care: Angeles University Foundation Angeles City College of Nursing SY 2010-1011Dokument23 SeitenWritten Report Prenatal Care: Angeles University Foundation Angeles City College of Nursing SY 2010-1011Mylene Angelie Bognot0% (1)
- Potayre, Shelomith Marie E. BSN Ii - H: Nursing Skills Output "Contraction Stress Test" DefinitionDokument3 SeitenPotayre, Shelomith Marie E. BSN Ii - H: Nursing Skills Output "Contraction Stress Test" DefinitionMarie PotayreNoch keine Bewertungen
- Prenatal care guideDokument31 SeitenPrenatal care guideNoraNoch keine Bewertungen
- 11 - Management of Labour & Fetal AssessmenDokument77 Seiten11 - Management of Labour & Fetal AssessmenGreen ArrowNoch keine Bewertungen
- 9 Antepartum CareDokument24 Seiten9 Antepartum CareFlowerer ShafaaNoch keine Bewertungen
- 2.induction of Labour & Prolonged PregnancyDokument20 Seiten2.induction of Labour & Prolonged PregnancyMiswar Abdul HalimNoch keine Bewertungen
- Preparing For DeliveryDokument27 SeitenPreparing For DeliveryKalpesh DalviNoch keine Bewertungen
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-IDokument6 SeitenGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (1)
- Induction of Labor 1Dokument36 SeitenInduction of Labor 1Jessy JoltuwuNoch keine Bewertungen
- Stages of LaborDokument3 SeitenStages of LaborShyla mayNoch keine Bewertungen
- Basic Emergency Obstetric CareDokument5 SeitenBasic Emergency Obstetric Caregabriel_marapaoNoch keine Bewertungen
- Stages of LaborDokument5 SeitenStages of LaborL Rean Carmelle MAGALLONES100% (1)
- AntepartumDokument128 SeitenAntepartumIris Caberte100% (1)
- ANC Ahmedhaji DocumentsDokument34 SeitenANC Ahmedhaji Documentsahmedhaji_sadik100% (1)
- Nursing Case Analysis 4Dokument3 SeitenNursing Case Analysis 4Luna GrayNoch keine Bewertungen
- Integrated Management of Childhood IllnessDokument16 SeitenIntegrated Management of Childhood IllnessSabrina Porquiado Magañan SNNoch keine Bewertungen
- JINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioDokument13 SeitenJINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioJashtine JingcoNoch keine Bewertungen
- Case Study For OB Skills DocxDokument14 SeitenCase Study For OB Skills DocxMaica QuilangNoch keine Bewertungen
- Assessing preterm labor risk in a pregnant patientDokument3 SeitenAssessing preterm labor risk in a pregnant patientCathy Marie Constante100% (1)
- Done, Normal Findings, Danger FindingsDokument4 SeitenDone, Normal Findings, Danger FindingsJoshua LadagaNoch keine Bewertungen
- Labor and Delivery Case PresentationDokument29 SeitenLabor and Delivery Case PresentationJoshua ABNoch keine Bewertungen
- Pregnancy Diagnosis and Fetal AssessmentDokument41 SeitenPregnancy Diagnosis and Fetal AssessmentKrystel Anne MilanNoch keine Bewertungen
- NSO (Nipple Stimulation Contraction Stress Test) SANAANIDokument5 SeitenNSO (Nipple Stimulation Contraction Stress Test) SANAANINur SetsuNoch keine Bewertungen
- Preterm LaborDokument18 SeitenPreterm LaborJezreel NicolasNoch keine Bewertungen
- Case Study #117Dokument4 SeitenCase Study #117Cheska Paloma100% (1)
- NCLEX-RN Questions: The Birth ExperienceDokument27 SeitenNCLEX-RN Questions: The Birth Experienceapi-323040992Noch keine Bewertungen
- Mother Baby Final Exam ReviewDokument14 SeitenMother Baby Final Exam ReviewAngelina mendezNoch keine Bewertungen
- Full Test BankDokument1 SeiteFull Test Bankjwjimmy20Noch keine Bewertungen
- Preventive Obstetrics SeminarDokument25 SeitenPreventive Obstetrics SeminarAnju MargaretNoch keine Bewertungen
- NCM 104 Lec Reviewer FinalsDokument11 SeitenNCM 104 Lec Reviewer FinalsFERNANDEZ, RELLY ANDREWNoch keine Bewertungen
- Seminar on Preventive Obstetrics MeasuresDokument50 SeitenSeminar on Preventive Obstetrics Measuressalmanhabeebek85% (13)
- High Risk PregnancyDokument113 SeitenHigh Risk PregnancyVivian Lajara100% (2)
- Antenatal Care Unit Two Lesson 192Dokument192 SeitenAntenatal Care Unit Two Lesson 192RidiculouslySweetNoch keine Bewertungen
- NCM 107 5M Case Analysis PDFDokument9 SeitenNCM 107 5M Case Analysis PDFKisha BethelNoch keine Bewertungen
- Preterm LabourDokument7 SeitenPreterm LabourAlana CaballeroNoch keine Bewertungen
- Preterm Labor & Cervical ProblemsDokument44 SeitenPreterm Labor & Cervical ProblemsDianna Rose AmigoNoch keine Bewertungen
- Maternity Evolve ExamDokument36 SeitenMaternity Evolve Examfriendofnurse100% (26)
- Monitoring Labor RisksDokument14 SeitenMonitoring Labor RisksShyla ManguiatNoch keine Bewertungen
- 092415l DassessmentDokument10 Seiten092415l Dassessmentapi-308634551Noch keine Bewertungen
- Promoting Maternal and Fetal WellnessDokument3 SeitenPromoting Maternal and Fetal WellnessKarl Kiw-isNoch keine Bewertungen
- Induction of LabourDokument25 SeitenInduction of LabourMohnnad Hmood AlgaraybhNoch keine Bewertungen
- S Preterm Birth and PromDokument6 SeitenS Preterm Birth and PromThembeka MbathaNoch keine Bewertungen
- Normal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraDokument13 SeitenNormal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraChatora Tsitsi VimbayiNoch keine Bewertungen
- Manage Complications of Labor and DeliveryDokument7 SeitenManage Complications of Labor and DeliveryMon Russel FriasNoch keine Bewertungen
- Antenatal Care AssessmentDokument67 SeitenAntenatal Care Assessmenthiral mistry100% (2)
- Drugs that Affect the Reproductive SystemDokument5 SeitenDrugs that Affect the Reproductive Systemjanina mykaNoch keine Bewertungen
- Cesearean Section FinalDokument62 SeitenCesearean Section FinalsanthiyasandyNoch keine Bewertungen
- CPC ON Twin PregnancyDokument23 SeitenCPC ON Twin PregnancyAyesha AsifNoch keine Bewertungen
- An Unplanned Interruption of Pregnancy Before The Fetus Is Viable. 3. Hypertension of Pregnancy That Involves Hemolysis, High LiverDokument3 SeitenAn Unplanned Interruption of Pregnancy Before The Fetus Is Viable. 3. Hypertension of Pregnancy That Involves Hemolysis, High LiverDyan Bianca Suaso LastimosaNoch keine Bewertungen
- Challenge Enteral Feeding Sga - RinawatiDokument17 SeitenChallenge Enteral Feeding Sga - RinawatiSuryani MalikNoch keine Bewertungen
- Maternity Investigation ReportDokument35 SeitenMaternity Investigation ReportRaluca GiurgiuNoch keine Bewertungen
- Weight Percentiles CalculatorDokument1 SeiteWeight Percentiles CalculatorAqila MumtazNoch keine Bewertungen
- KGN Hospital Test Tube Baby LaturDokument35 SeitenKGN Hospital Test Tube Baby LaturDr Aamir ShaikhNoch keine Bewertungen
- First Versus Second Trimester Mean Platelet Volume and Uric Acid For Prediction of Preeclampsia in Women at Moderate and Low RiskDokument8 SeitenFirst Versus Second Trimester Mean Platelet Volume and Uric Acid For Prediction of Preeclampsia in Women at Moderate and Low RiskWael GaberNoch keine Bewertungen
- Weight For Height As A Measure of Nutritional Status in Filipino Pregnant WomenDokument9 SeitenWeight For Height As A Measure of Nutritional Status in Filipino Pregnant WomenCecilia AcuinNoch keine Bewertungen
- AnencephalyDokument2 SeitenAnencephalysrust2792Noch keine Bewertungen
- Faktor Yang Berhubungan Dengan Kesiapan Persalinan Ibu Primigravida Di Wilayah Kerja Puskesmas Batulappa Kabupaten PinrangDokument5 SeitenFaktor Yang Berhubungan Dengan Kesiapan Persalinan Ibu Primigravida Di Wilayah Kerja Puskesmas Batulappa Kabupaten PinrangPapy AleshaNoch keine Bewertungen
- Everything You Need to Know About C-SectionsDokument46 SeitenEverything You Need to Know About C-SectionsBugingo Julita100% (2)
- Individual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerDokument11 SeitenIndividual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerSatanichia McDowell KurumizawaNoch keine Bewertungen
- APH&PPHDokument77 SeitenAPH&PPHKåbåñå TürüñåNoch keine Bewertungen
- Prevalence of High Risk Pregnancy in Rural DharwadDokument4 SeitenPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNoch keine Bewertungen
- Maternal Hemoglobin Concentration and Birth Weight: Philip J SteerDokument3 SeitenMaternal Hemoglobin Concentration and Birth Weight: Philip J Steerriza210488Noch keine Bewertungen
- Biophysical Profile PDFDokument8 SeitenBiophysical Profile PDFHans Cifuentes VillatoroNoch keine Bewertungen
- Risk Factors for Low Birth Weight in MalaysiaDokument5 SeitenRisk Factors for Low Birth Weight in Malaysiaerine5995Noch keine Bewertungen
- Pregnancy Assessment Health History ROSDokument34 SeitenPregnancy Assessment Health History ROSteuuuuNoch keine Bewertungen
- Mcqs Test Unit 8 With KeyDokument5 SeitenMcqs Test Unit 8 With Keyyasodha maharajNoch keine Bewertungen
- History of Motherhood Package InitiativeDokument3 SeitenHistory of Motherhood Package Initiativetaizya cNoch keine Bewertungen
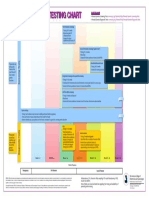
- Prenatal Genetic Testing ChartDokument1 SeitePrenatal Genetic Testing ChartMorningDewNoch keine Bewertungen
- Vaginal Birth After Cesarean: New Insights: Evidence Report/Technology AssessmentDokument397 SeitenVaginal Birth After Cesarean: New Insights: Evidence Report/Technology AssessmentRizki IrwansyahNoch keine Bewertungen
- MCHN Midterm ReviewerDokument24 SeitenMCHN Midterm Reviewerpat delapenaNoch keine Bewertungen
- ReportDokument7 SeitenReportAnchalNoch keine Bewertungen
- Antenatal Cardiotocography For Fetal Assessment (Review) : Grivell RM, Alfirevic Z, Gyte GML, Devane DDokument50 SeitenAntenatal Cardiotocography For Fetal Assessment (Review) : Grivell RM, Alfirevic Z, Gyte GML, Devane DDara Loor GonzálesNoch keine Bewertungen
- Efektivitas Buah Pisang Ambon Terhadap Tekanan Darah Ibu Hamil HipertensiDokument6 SeitenEfektivitas Buah Pisang Ambon Terhadap Tekanan Darah Ibu Hamil Hipertensihas hasriadiNoch keine Bewertungen
- Herreria, Hannah U. BSN 2 N038Dokument2 SeitenHerreria, Hannah U. BSN 2 N038Hannah Urmeneta HerreriaNoch keine Bewertungen
- Preconceptional Counseling and CareDokument12 SeitenPreconceptional Counseling and CareGaurav ThakurNoch keine Bewertungen
- Cerebroplacental Ratio in Fetal Well Being Assessment in SGA and AGA FetusDokument11 SeitenCerebroplacental Ratio in Fetal Well Being Assessment in SGA and AGA FetuspolygoneNoch keine Bewertungen