Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Design Project: SEV200 - Geotechnical Investigation and Design Last Update: 09/05/2020Dokument12 SeitenDesign Project: SEV200 - Geotechnical Investigation and Design Last Update: 09/05/2020abdulqadirghoriNoch keine Bewertungen
- Mechanics of Solids: Bela I. Sandor Ryan Roloff Stephen M. Birn Maan H. Jawad Michael L. BrownDokument1 SeiteMechanics of Solids: Bela I. Sandor Ryan Roloff Stephen M. Birn Maan H. Jawad Michael L. BrownkprasannanNoch keine Bewertungen
- Aditya and VarahaDokument7 SeitenAditya and VarahaVibhats VibhorNoch keine Bewertungen
- Design Guide Handbook For EN 1996 Design of Masonry StructuresDokument46 SeitenDesign Guide Handbook For EN 1996 Design of Masonry Structuresbusyspider100% (1)
- A2 Nuclear Models LiqDrop FermiGasDokument19 SeitenA2 Nuclear Models LiqDrop FermiGasAbdul RehmanNoch keine Bewertungen
- Spectrophotometric Determination of The Equilibrium Constant of A ReactionDokument5 SeitenSpectrophotometric Determination of The Equilibrium Constant of A Reactionnarras11100% (1)
- Hiad 2Dokument15 SeitenHiad 2Hrishikesh JoshiNoch keine Bewertungen
- Physics Precision Measurement ReportDokument7 SeitenPhysics Precision Measurement ReportBramwel Mbogo78% (76)
- Tensile Strength of Mass Concrete 913-938 PDFDokument28 SeitenTensile Strength of Mass Concrete 913-938 PDFchutton681Noch keine Bewertungen
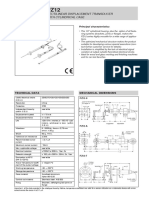
- Rectilinear Displacement Transducer With Cylindrical Case: Technical Data Mechanical DimensionsDokument2 SeitenRectilinear Displacement Transducer With Cylindrical Case: Technical Data Mechanical Dimensionsl561926Noch keine Bewertungen
- Dr. Mezmer's Psychopedia of Bad PsychologyDokument378 SeitenDr. Mezmer's Psychopedia of Bad PsychologyArt Marr100% (5)
- Functional Requirements and Concepts of Frequency Converter's Oil Application Control ProgramDokument78 SeitenFunctional Requirements and Concepts of Frequency Converter's Oil Application Control ProgramRigoberto José Martínez CedeñoNoch keine Bewertungen
- Long Term Deflection in Concrete BeamsDokument6 SeitenLong Term Deflection in Concrete BeamsRenganayagi BalajiNoch keine Bewertungen
- Engineering Structures: SciencedirectDokument12 SeitenEngineering Structures: Sciencedirectyasemin bürüngüzNoch keine Bewertungen
- Jet Bit Nozzle Size SelectionDokument46 SeitenJet Bit Nozzle Size SelectionBharat BhattaraiNoch keine Bewertungen
- Hammer, Harper, Ryan - 2001 - Past Paleontological Statistics Software Package For Education and Data AnalysisDokument7 SeitenHammer, Harper, Ryan - 2001 - Past Paleontological Statistics Software Package For Education and Data AnalysisA3A31234Noch keine Bewertungen
- Experimental Investigation of Process Parameters On Inconel 925 For EDM Process by Using Taguchi MethodDokument6 SeitenExperimental Investigation of Process Parameters On Inconel 925 For EDM Process by Using Taguchi MethodVishal Kumar JaiswalNoch keine Bewertungen
- E-DWT-H Electronic Deadweight TesterDokument2 SeitenE-DWT-H Electronic Deadweight TesterMorosanu Andreea-DianaNoch keine Bewertungen
- Ad 7746Dokument28 SeitenAd 7746pskorovsNoch keine Bewertungen
- ISO 3354 - 2008 Velocityarea MethodsDokument64 SeitenISO 3354 - 2008 Velocityarea MethodsM.C. Санников0% (1)
- Britishhomoeopat 00 BritialaDokument448 SeitenBritishhomoeopat 00 BritialaAlbena Trifonova0% (2)
- Gyro Notes For 2ND MateDokument18 SeitenGyro Notes For 2ND MateArchit Bhardwaj100% (1)
- Reciprocating compressor performance analysis using computer simulationDokument9 SeitenReciprocating compressor performance analysis using computer simulationLeandro Garcia VelaNoch keine Bewertungen
- Vacita Integrated ServicesDokument21 SeitenVacita Integrated ServicesNwosu AugustineNoch keine Bewertungen
- PDFDokument36 SeitenPDFvishwasdeepjoshiNoch keine Bewertungen
- M.Prasad Naidu MSC Medical Biochemistry, PH.D Research ScholarDokument31 SeitenM.Prasad Naidu MSC Medical Biochemistry, PH.D Research ScholarDr. M. Prasad NaiduNoch keine Bewertungen
- ANSYS Model of A Cylindrical Fused Silica Fibre-01Dokument15 SeitenANSYS Model of A Cylindrical Fused Silica Fibre-01lamia97Noch keine Bewertungen
- Ricapito-1 PbLi-T DatabaseDokument16 SeitenRicapito-1 PbLi-T DatabaseSasa DjordjevicNoch keine Bewertungen
- Temperature Regulator With Two Temperature SensorsDokument2 SeitenTemperature Regulator With Two Temperature SensorsSandi AslanNoch keine Bewertungen
- Name: Teacher: Date: Score:: Identify The Properties of MathematicsDokument2 SeitenName: Teacher: Date: Score:: Identify The Properties of MathematicsMacPapitaNoch keine Bewertungen