Das könnte Ihnen auch gefallen
- A Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeVon EverandA Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeNoch keine Bewertungen
- Assessing Uptake of National HIV Screening and Testing Guidance-Part 2: Knowledge, Comfort and PracticeDokument9 SeitenAssessing Uptake of National HIV Screening and Testing Guidance-Part 2: Knowledge, Comfort and PracticeIrna SulistiyaniNoch keine Bewertungen
- Vih Ingreso Al Cuidado VihDokument15 SeitenVih Ingreso Al Cuidado Vihsamuro625Noch keine Bewertungen
- NIH Public Access: Provider-Initiated HIV Testing and Counseling in Low-And Middle-Income Countries: A Systematic ReviewDokument20 SeitenNIH Public Access: Provider-Initiated HIV Testing and Counseling in Low-And Middle-Income Countries: A Systematic ReviewAlexandra PaunNoch keine Bewertungen
- n594 D Program Theory PaperDokument16 Seitenn594 D Program Theory Paperapi-272730495Noch keine Bewertungen
- Policy BriefDokument8 SeitenPolicy BriefWendy DixonNoch keine Bewertungen
- Artigo Sobre AidsDokument7 SeitenArtigo Sobre AidscamilatututNoch keine Bewertungen
- NCAAN and DHJC Medicaid CommentsDokument61 SeitenNCAAN and DHJC Medicaid CommentsLee StorrowNoch keine Bewertungen
- Pediatrics 2012 Fu E496 503jnnjnjnjDokument10 SeitenPediatrics 2012 Fu E496 503jnnjnjnjDyera JessenskyNoch keine Bewertungen
- Economics Case Study AnalysisDokument4 SeitenEconomics Case Study AnalysisMustafa MahmoodNoch keine Bewertungen
- Burmen B, Mutai K: Abstract-Linkage of Newly Diagnosed HIV Positive IndividualsDokument9 SeitenBurmen B, Mutai K: Abstract-Linkage of Newly Diagnosed HIV Positive IndividualsJASH MATHEWNoch keine Bewertungen
- 67-1426444406 FinalPublishedVersion PDFDokument16 Seiten67-1426444406 FinalPublishedVersion PDFSandi BongNoch keine Bewertungen
- HIV-related Stigma and DiscriminationDokument11 SeitenHIV-related Stigma and DiscriminationRey Ann PangilinanNoch keine Bewertungen
- POC Testing For HCV at CBOsDokument1 SeitePOC Testing For HCV at CBOsRobert G. Gish, MDNoch keine Bewertungen
- Does A Clinical Guideline Change Chlamydia Testing?Dokument7 SeitenDoes A Clinical Guideline Change Chlamydia Testing?gt_shadowNoch keine Bewertungen
- Nhs Health Check Programme Literature ReviewDokument6 SeitenNhs Health Check Programme Literature Reviewafmzzantalfbfa100% (1)
- Researcharticle Open AccessDokument14 SeitenResearcharticle Open AccessHIV Justice NetworkNoch keine Bewertungen
- En HIV Screening Guide 2013Dokument57 SeitenEn HIV Screening Guide 2013radersNoch keine Bewertungen
- Dissction Unit 3Dokument2 SeitenDissction Unit 3hgfyfNoch keine Bewertungen
- DRAFT 2016 Letter To Issuers in The Federally-Facilitated MarketplacesDokument6 SeitenDRAFT 2016 Letter To Issuers in The Federally-Facilitated MarketplacesRobert G. Gish, MDNoch keine Bewertungen
- Behavioural Interventions EngDokument6 SeitenBehavioural Interventions EngMatin Ahmad KhanNoch keine Bewertungen
- Vih GuidlineDokument21 SeitenVih GuidlineDavid MonroyNoch keine Bewertungen
- SC 10Dokument16 SeitenSC 10khamilatusyNoch keine Bewertungen
- IDweek Poster No397 Final CorrectedDokument1 SeiteIDweek Poster No397 Final CorrectedanaluvcNoch keine Bewertungen
- Rapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Dokument5 SeitenRapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Elisa BaronNoch keine Bewertungen
- Executive Summary: Blueprint For Harm Reduction Coalition Ilanna S Mandel, 2008Dokument5 SeitenExecutive Summary: Blueprint For Harm Reduction Coalition Ilanna S Mandel, 2008IlannaNoch keine Bewertungen
- 10.1186@s13643-015-0136-x Sistematik ReviewDokument6 Seiten10.1186@s13643-015-0136-x Sistematik ReviewAnonymous tmw24cW0Noch keine Bewertungen
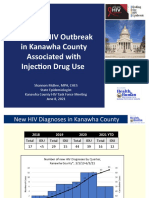
- Update: HIV Outbreak in Kanawha County Associated With Injection Drug UseDokument10 SeitenUpdate: HIV Outbreak in Kanawha County Associated With Injection Drug UseJune LefflerNoch keine Bewertungen
- Literature Review On Hiv Counselling and TestingDokument4 SeitenLiterature Review On Hiv Counselling and Testingwopugemep0h3100% (1)
- Public Health Ambulatory Services - CH 5Dokument2 SeitenPublic Health Ambulatory Services - CH 5Pranav ParsiNoch keine Bewertungen
- Journal Pone 0250434Dokument35 SeitenJournal Pone 0250434Aklilu FelekeNoch keine Bewertungen
- The Intertwined Epidemics of Hiv TBDokument2 SeitenThe Intertwined Epidemics of Hiv TBSaikat DattaNoch keine Bewertungen
- From Caution To UrgencyDokument6 SeitenFrom Caution To UrgencyadrieanaNoch keine Bewertungen
- HIV Screening USPTFDokument21 SeitenHIV Screening USPTFhivpolicyyesNoch keine Bewertungen
- Collective Call To Action For HIVAIDS Community Based CollaborativeDokument4 SeitenCollective Call To Action For HIVAIDS Community Based CollaborativeKristiani AmbengNoch keine Bewertungen
- art3A10.10072Fs10461 015 1097 8Dokument18 Seitenart3A10.10072Fs10461 015 1097 8Aklilu FelekeNoch keine Bewertungen
- 2.3 HontelezDokument12 Seiten2.3 Hontelezallan.manaloto23Noch keine Bewertungen
- Ppa 6 457 PDFDokument7 SeitenPpa 6 457 PDFElizabeth SniderNoch keine Bewertungen
- Guide-Clinical-Preventive-Services 2012Dokument128 SeitenGuide-Clinical-Preventive-Services 2012Gem BorjaNoch keine Bewertungen
- Improving Diagnosis in Health CareDokument4 SeitenImproving Diagnosis in Health CareHLMedit100% (1)
- Mapping The Effectiveness of Integrating Mental Health in HIV Programs - A Scoping Review - 2023Dokument14 SeitenMapping The Effectiveness of Integrating Mental Health in HIV Programs - A Scoping Review - 2023Ashik RahamanNoch keine Bewertungen
- Bentuk-Bentuk NegaraDokument48 SeitenBentuk-Bentuk NegaraMas Yudha WaeNoch keine Bewertungen
- Hiv ProphylaxisDokument193 SeitenHiv ProphylaxisKiran MishraNoch keine Bewertungen
- !!!!!! HivDokument8 Seiten!!!!!! HivNela PopaNoch keine Bewertungen
- Hep C 2017Dokument11 SeitenHep C 2017Rahadian MalikNoch keine Bewertungen
- Policy and Public Health: Reducing The Burden of Infectious DiseasesDokument5 SeitenPolicy and Public Health: Reducing The Burden of Infectious DiseasesPriyanka MishraNoch keine Bewertungen
- Initiation of ARV Treatment Protects Uninfected Sexual Partners From HIV (HPTN Study 052)Dokument2 SeitenInitiation of ARV Treatment Protects Uninfected Sexual Partners From HIV (HPTN Study 052)Laura Lopez GonzalezNoch keine Bewertungen
- Health Policy Brief - FinalDokument5 SeitenHealth Policy Brief - Finalapi-315325454Noch keine Bewertungen
- Perceptions Dynamics About Antiretroviral Treatment Among HIV Patients in BaliDokument8 SeitenPerceptions Dynamics About Antiretroviral Treatment Among HIV Patients in BaliIJPHSNoch keine Bewertungen
- Pediatric Cancer SurvivorshipDokument315 SeitenPediatric Cancer SurvivorshipRJ HSNoch keine Bewertungen
- Outcomes Approaches and Challenges To Developing and Passing A Contrywide Mandatory Vaccinationpolicu ST Louis Hep ADokument15 SeitenOutcomes Approaches and Challenges To Developing and Passing A Contrywide Mandatory Vaccinationpolicu ST Louis Hep ANancy KawilarangNoch keine Bewertungen
- Uma Intervenção Clínica Realizada Por Enfermeiros para Tratar Da Violência Por Parceiro Íntimo Entre Mulheres de Baixa Renda Na Cidade Do MéxicoDokument12 SeitenUma Intervenção Clínica Realizada Por Enfermeiros para Tratar Da Violência Por Parceiro Íntimo Entre Mulheres de Baixa Renda Na Cidade Do MéxicoLorrany Prado QuirinoNoch keine Bewertungen
- Da ThesisDokument3 SeitenDa ThesisAkhirah MagkilatNoch keine Bewertungen
- SOP - HIV Care Patient Follow-Up ProgrammeDokument23 SeitenSOP - HIV Care Patient Follow-Up ProgrammeParwatiNoch keine Bewertungen
- DarenoDokument14 SeitenDarenoguohong huNoch keine Bewertungen
- 2020 Comparing The Effects of HIV Self-Testing To Standard HIV Testing For Key Populations A Systematic Review and Meta-AnalysisDokument13 Seiten2020 Comparing The Effects of HIV Self-Testing To Standard HIV Testing For Key Populations A Systematic Review and Meta-AnalysisAmalia Candela De LucaNoch keine Bewertungen
- New Guidelines On HIV Prevention in Teens and AdultsDokument1 SeiteNew Guidelines On HIV Prevention in Teens and AdultsFadhilah M. YanuarNoch keine Bewertungen
- Screening para HivDokument12 SeitenScreening para HivNuñez Fonseca JoseNoch keine Bewertungen
- 12MoContinuousEligibilityUtilization Final 4pgDokument4 Seiten12MoContinuousEligibilityUtilization Final 4pgSHADACNoch keine Bewertungen
- Cost Effectiveness of A Care Program For HIV AIDS Patients - 2016 - Value in HeDokument8 SeitenCost Effectiveness of A Care Program For HIV AIDS Patients - 2016 - Value in HeSansa LauraNoch keine Bewertungen
- 9Dokument6 Seiten9Leon L GayaNoch keine Bewertungen
- Is Albumin Use SAFE in Patients With Traumatic Brain Injury?Dokument3 SeitenIs Albumin Use SAFE in Patients With Traumatic Brain Injury?Leon L GayaNoch keine Bewertungen
- 1Dokument12 Seiten1Leon L GayaNoch keine Bewertungen
- 2014 Intravenous Fluids en Traumatic Bran Injury PDFDokument3 Seiten2014 Intravenous Fluids en Traumatic Bran Injury PDFWilmer Yanquen VillarrealNoch keine Bewertungen
- 7Dokument7 Seiten7Leon L GayaNoch keine Bewertungen
- 10Dokument15 Seiten10Leon L GayaNoch keine Bewertungen
- 2Dokument11 Seiten2Leon L GayaNoch keine Bewertungen
- Digestive SsDokument46 SeitenDigestive SsLeon L GayaNoch keine Bewertungen
- Hamid Et Al AntioksidanDokument10 SeitenHamid Et Al AntioksidanDjihan Ryn PratiwiNoch keine Bewertungen
- Androgen-Antiandrogen - DR Asep SukoharDokument61 SeitenAndrogen-Antiandrogen - DR Asep SukoharLeon L GayaNoch keine Bewertungen
- Hamid Et Al AntioksidanDokument10 SeitenHamid Et Al AntioksidanDjihan Ryn PratiwiNoch keine Bewertungen
- BPH-erectile Dysfunction PharmacotherapyDokument32 SeitenBPH-erectile Dysfunction PharmacotherapyLeon L GayaNoch keine Bewertungen
- 1472 6882 13 56 PDFDokument17 Seiten1472 6882 13 56 PDFLeon L GayaNoch keine Bewertungen
- Examination of The Eyes Teaching SetDokument19 SeitenExamination of The Eyes Teaching SetLeon L GayaNoch keine Bewertungen
- Management of Acute Variceal Bleeding Using Hemostatic PowderDokument7 SeitenManagement of Acute Variceal Bleeding Using Hemostatic PowderLeon L GayaNoch keine Bewertungen
- DAPUSDokument6 SeitenDAPUSLeon L GayaNoch keine Bewertungen
- Asma IdiDokument69 SeitenAsma IdimetidesNoch keine Bewertungen
- AnthraxDokument20 SeitenAnthraxLeon L GayaNoch keine Bewertungen
- Employment and Activity Limitations Among Adults With Chronic Obstructive Pulmonary Disease - United States, 2013Dokument24 SeitenEmployment and Activity Limitations Among Adults With Chronic Obstructive Pulmonary Disease - United States, 2013Leon L GayaNoch keine Bewertungen
- BrucellosisDokument30 SeitenBrucellosisLeon L GayaNoch keine Bewertungen
- Sport Injuries and ManagementsDokument59 SeitenSport Injuries and ManagementsLeon L GayaNoch keine Bewertungen
- NIH Public Access: Treatment As Prevention-Where Next?Dokument15 SeitenNIH Public Access: Treatment As Prevention-Where Next?Leon L GayaNoch keine Bewertungen
- Basic BiomechanicDokument83 SeitenBasic BiomechanicGarrett SimpsonNoch keine Bewertungen
- Nihms 680774Dokument21 SeitenNihms 680774Leon L GayaNoch keine Bewertungen
- m2 l5 Evaluation and Prognosis of Patients With CirrhosisDokument17 Seitenm2 l5 Evaluation and Prognosis of Patients With CirrhosisLeon L GayaNoch keine Bewertungen
- Pseudomonas AeruginosaDokument7 SeitenPseudomonas AeruginosaLeon L GayaNoch keine Bewertungen
- Child Pugh ScoreDokument1 SeiteChild Pugh ScoreRyoFernandoNoch keine Bewertungen
- Techniques of TIPS in The Treatment of Liver Cirrhosis Combined With Incompletely Occlusive Main Portal Vein ThrombosisDokument9 SeitenTechniques of TIPS in The Treatment of Liver Cirrhosis Combined With Incompletely Occlusive Main Portal Vein ThrombosisLeon L GayaNoch keine Bewertungen
- Transposition of The Great ArteriesDokument118 SeitenTransposition of The Great ArteriesJoan Rae Tan100% (1)
- AXA - Sales Brochure Qatar - ALL - ENDokument10 SeitenAXA - Sales Brochure Qatar - ALL - ENAhmad MuhammadNoch keine Bewertungen
- 7981bc6c PDFDokument8 Seiten7981bc6c PDFGungaa JaltsanNoch keine Bewertungen
- Roleplay Discharge PlanningDokument3 SeitenRoleplay Discharge PlanningAnonymous KQKONmD9H100% (1)
- Project CharterDokument9 SeitenProject CharterTatianaObregon100% (1)
- CARESCAPE Monitor B650: Clinical Reference ManualDokument210 SeitenCARESCAPE Monitor B650: Clinical Reference ManualJonathan ScottNoch keine Bewertungen
- Rogelio Ramos Vs CADokument28 SeitenRogelio Ramos Vs CAAnonymous FBDGfUqHENoch keine Bewertungen
- Telehealth Research and Evaluation Implications For Decision MakersDokument9 SeitenTelehealth Research and Evaluation Implications For Decision Makerscharlsandroid01Noch keine Bewertungen
- EU Digital COVID Certificate Certificat Digital European COVIDDokument2 SeitenEU Digital COVID Certificate Certificat Digital European COVIDDespre FotografieNoch keine Bewertungen
- 1mg PrescriptionDokument2 Seiten1mg PrescriptionSankalp IN GamingNoch keine Bewertungen
- Studi Kasus: Kehamilan Dengan: Dengan Katub Jantung Prostetik Mekanik Dan Penggunaan AntikoagulanDokument10 SeitenStudi Kasus: Kehamilan Dengan: Dengan Katub Jantung Prostetik Mekanik Dan Penggunaan AntikoagulanMonyet...Noch keine Bewertungen
- Growing The Mandible? Impossible, Right?: SpecialDokument4 SeitenGrowing The Mandible? Impossible, Right?: SpecialAriana Moreno ZavalaNoch keine Bewertungen
- The Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityDokument25 SeitenThe Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityGian Alodia RisamasuNoch keine Bewertungen
- Medicinal PlantsDokument214 SeitenMedicinal PlantsArnold Jr Bautista100% (1)
- Links To Clinical Info About The VaccineDokument9 SeitenLinks To Clinical Info About The VaccinekarunaNoch keine Bewertungen
- El Paso Harm Reduction Alliance PresentationDokument20 SeitenEl Paso Harm Reduction Alliance PresentationFallon FischerNoch keine Bewertungen
- American Health National Security (HNS) Issue Omission Resolution Green Paper CD Fax Version 5-07-2010Dokument66 SeitenAmerican Health National Security (HNS) Issue Omission Resolution Green Paper CD Fax Version 5-07-2010George SingletonNoch keine Bewertungen
- Lecture1 2 Advancedemergencytraumacourse Introductionandcourseoverview 1Dokument66 SeitenLecture1 2 Advancedemergencytraumacourse Introductionandcourseoverview 1vikoraNoch keine Bewertungen
- Rotavirus SD BIOLINE BrochureDokument1 SeiteRotavirus SD BIOLINE BrochureLabor KaruniaNoch keine Bewertungen
- Testicular Torsion Torsio TestisDokument34 SeitenTesticular Torsion Torsio TestisAira Kelly50% (2)
- Exam Semi23423123132Dokument2 SeitenExam Semi23423123132gwapoNoch keine Bewertungen
- Baca EKG Yok: Fenda Adita, 2012Dokument45 SeitenBaca EKG Yok: Fenda Adita, 2012SarahNoch keine Bewertungen
- Gestational Diabetes MellitusDokument11 SeitenGestational Diabetes Mellitusjohn jumborockNoch keine Bewertungen
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDokument24 SeitenNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarNoch keine Bewertungen
- Tutor: Dr. Vera Dr. Haerani: Skenario Problems Learning Objectives Main Map ReferensiDokument36 SeitenTutor: Dr. Vera Dr. Haerani: Skenario Problems Learning Objectives Main Map ReferensiAdeLia Nur FitrianaNoch keine Bewertungen
- High Blood Pressure Screening PackageDokument1 SeiteHigh Blood Pressure Screening PackageAlita PalpialyNoch keine Bewertungen
- Aspirin (Plus Antiplatelet Medicines) - What Is Aspirin - PatientDokument9 SeitenAspirin (Plus Antiplatelet Medicines) - What Is Aspirin - Patientaasuman123Noch keine Bewertungen
- PneumoniaDokument27 SeitenPneumoniamameekasim75Noch keine Bewertungen
- Determination of Risk Factors For Drug - Related Problems - A Multidisciplinary Triangulation ProcessDokument7 SeitenDetermination of Risk Factors For Drug - Related Problems - A Multidisciplinary Triangulation Processzenita reizaNoch keine Bewertungen
- First Aid - CPR - AED Participant's ManualDokument196 SeitenFirst Aid - CPR - AED Participant's Manualadamiam100% (2)