Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- M Selvam Fabrication SupervisorDokument4 SeitenM Selvam Fabrication SupervisornaguNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- RFI For Welding Inspection EJN00048Dokument1 SeiteRFI For Welding Inspection EJN00048nagu100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- M Selvam Fabrication FORMENDokument4 SeitenM Selvam Fabrication FORMENnaguNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Sudip Kumar Jana: Application Applied For Pipe FabricatorDokument2 SeitenSudip Kumar Jana: Application Applied For Pipe FabricatornaguNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Material Rfi, Test Report-30122016104619 PDFDokument2 SeitenMaterial Rfi, Test Report-30122016104619 PDFnagu100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Material Rfi & Hydro Test ReportDokument2 SeitenMaterial Rfi & Hydro Test Reportnagu100% (1)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
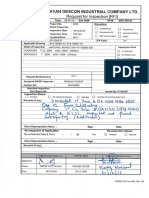
- Olayan Descon Industrial Company LTD.: Request For Inspection (RFI)Dokument1 SeiteOlayan Descon Industrial Company LTD.: Request For Inspection (RFI)naguNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- 16 - Work Place StressDokument10 Seiten16 - Work Place StressnaguNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Golden Joint 100% PT (Root & Final Weld) FW-01, FW-02, FW-08ADokument2 SeitenGolden Joint 100% PT (Root & Final Weld) FW-01, FW-02, FW-08AnaguNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Weekly Welding Rejection RateDokument1 SeiteWeekly Welding Rejection Ratenagu100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- New 2016 NDT Handbook Vol 10 2 PDFDokument600 SeitenNew 2016 NDT Handbook Vol 10 2 PDFnagu100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Gate PassDokument90 SeitenGate PassnaguNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Safety Presentation 1Dokument1 SeiteSafety Presentation 1naguNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- EHS Observtios For Flare Project DCS On 03 08 16Dokument41 SeitenEHS Observtios For Flare Project DCS On 03 08 16naguNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- SAFETY Action Plan For 2016Dokument6 SeitenSAFETY Action Plan For 2016naguNoch keine Bewertungen
- 2 Welding TerminologyDokument26 Seiten2 Welding TerminologynaguNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 03 & 04 Duties of SWI and QualityDokument59 Seiten03 & 04 Duties of SWI and Qualitynagu100% (1)
- Cswip 3.2 Drawing ReviewDokument6 SeitenCswip 3.2 Drawing Reviewnagu75% (4)
- ALE Manual For LaserScope Arc Lamp Power SupplyDokument34 SeitenALE Manual For LaserScope Arc Lamp Power SupplyKen DizzeruNoch keine Bewertungen
- To Find Fatty Material of Different Soap SamplesDokument17 SeitenTo Find Fatty Material of Different Soap SamplesRohan Singh0% (2)
- Form Expense ClaimDokument2 SeitenForm Expense Claimviedelamonde_3868443Noch keine Bewertungen
- Ajmera - Treon - FF - R4 - 13-11-17 FinalDokument45 SeitenAjmera - Treon - FF - R4 - 13-11-17 FinalNikita KadamNoch keine Bewertungen
- Phylogeny Practice ProblemsDokument3 SeitenPhylogeny Practice ProblemsSusan Johnson100% (1)
- 1 Bacterial DeseaseDokument108 Seiten1 Bacterial DeseasechachaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Advertising II Marathi VersionDokument91 SeitenAdvertising II Marathi VersionHarsh Sangani100% (1)
- Mathematics BQP 2022Dokument43 SeitenMathematics BQP 2022muhammadmansuri815Noch keine Bewertungen
- Arduino Uno CNC ShieldDokument11 SeitenArduino Uno CNC ShieldMărian IoanNoch keine Bewertungen
- Upes School of Law Lac & Adr Association: PresentsDokument7 SeitenUpes School of Law Lac & Adr Association: PresentsSuvedhya ReddyNoch keine Bewertungen
- Bacacay South Hris1Dokument7.327 SeitenBacacay South Hris1Lito ObstaculoNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Эквивалентная Схема Мотра Теслы с Thomas2020Dokument7 SeitenЭквивалентная Схема Мотра Теслы с Thomas2020Алексей ЯмаNoch keine Bewertungen
- CN1111 Tutorial 4 QuestionDokument3 SeitenCN1111 Tutorial 4 Questionthenewperson0% (1)
- Analytical Chem Lab #3Dokument4 SeitenAnalytical Chem Lab #3kent galangNoch keine Bewertungen
- Exotic DVM 11 3 CompleteDokument12 SeitenExotic DVM 11 3 CompleteLuc CardNoch keine Bewertungen
- Business-Communication Solved MCQs (Set-3)Dokument8 SeitenBusiness-Communication Solved MCQs (Set-3)Pavan Sai Krishna KottiNoch keine Bewertungen
- DION IMPACT 9102 SeriesDokument5 SeitenDION IMPACT 9102 SeriesLENEEVERSONNoch keine Bewertungen
- Network Fundamentas ITEC90Dokument5 SeitenNetwork Fundamentas ITEC90Psychopomp PomppompNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Manual E07ei1Dokument57 SeitenManual E07ei1EiriHouseNoch keine Bewertungen
- Hydro Electric Fire HistoryDokument3 SeitenHydro Electric Fire HistorygdmurfNoch keine Bewertungen
- Aditya Birla GroupDokument21 SeitenAditya Birla GroupNarendra ThummarNoch keine Bewertungen
- Google Tools: Reggie Luther Tracsoft, Inc. 706-568-4133Dokument23 SeitenGoogle Tools: Reggie Luther Tracsoft, Inc. 706-568-4133nbaghrechaNoch keine Bewertungen
- Transportasi Distribusi MigasDokument25 SeitenTransportasi Distribusi MigasDian Permatasari100% (1)
- Espree I Class Korr3Dokument22 SeitenEspree I Class Korr3hgaucherNoch keine Bewertungen
- FpsecrashlogDokument19 SeitenFpsecrashlogtim lokNoch keine Bewertungen
- SyncopeDokument105 SeitenSyncopeJohn DasNoch keine Bewertungen
- EKRP311 Vc-Jun2022Dokument3 SeitenEKRP311 Vc-Jun2022dfmosesi78Noch keine Bewertungen
- S4 HANALicensing Model External V19Dokument28 SeitenS4 HANALicensing Model External V19Edir JuniorNoch keine Bewertungen
- Satish Gujral - FinalDokument23 SeitenSatish Gujral - Finalsatya madhuNoch keine Bewertungen
- Binary OptionsDokument24 SeitenBinary Optionssamsa7Noch keine Bewertungen