Das könnte Ihnen auch gefallen
- Hepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostDokument10 SeitenHepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostNurul An NisaNoch keine Bewertungen
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeVon EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNoch keine Bewertungen
- SMART Asthma TherapyDokument4 SeitenSMART Asthma TherapyKen Won100% (1)
- Youth Stress EssayDokument3 SeitenYouth Stress EssayGemma100% (1)
- Cholangiocarcinoma: R.KarthikeyanDokument49 SeitenCholangiocarcinoma: R.KarthikeyanKarthikeyan R100% (2)
- CholangiocarcinomaDokument7 SeitenCholangiocarcinomailovedaneNoch keine Bewertungen
- Hepatocellular Carcinoma - Diagnosis and TreatmentDokument46 SeitenHepatocellular Carcinoma - Diagnosis and TreatmentSigh BalaNoch keine Bewertungen
- CholangiocarcinomaDokument9 SeitenCholangiocarcinomaloloalpsheidiNoch keine Bewertungen
- 10 1016@j CLD 2014 09 006Dokument23 Seiten10 1016@j CLD 2014 09 006Felix camilo GonzálezNoch keine Bewertungen
- Tumor GIT - Dr. Fanny 2020Dokument51 SeitenTumor GIT - Dr. Fanny 2020kintan 102017153Noch keine Bewertungen
- Squamous Cell Tumors Bile Duct Cancers: PathophysiologyDokument6 SeitenSquamous Cell Tumors Bile Duct Cancers: PathophysiologySiti RahmahNoch keine Bewertungen
- Cholangiocarcinoma 2 Juni 2018Dokument40 SeitenCholangiocarcinoma 2 Juni 2018Anonymous 1UgsHkUNoch keine Bewertungen
- It Is Not Always A Cholangiocarcinoma: Unusual Peritoneal Carcinomatosis Revealing Gastric AdenocarcinomaDokument5 SeitenIt Is Not Always A Cholangiocarcinoma: Unusual Peritoneal Carcinomatosis Revealing Gastric AdenocarcinomaIJAR JOURNALNoch keine Bewertungen
- Jordanian Surgical Society - PPT LastDokument166 SeitenJordanian Surgical Society - PPT LastNessreen Jamal100% (1)
- Cholangiocarcinoma - Radiology Reference Article - RadiopaediaDokument5 SeitenCholangiocarcinoma - Radiology Reference Article - RadiopaediaWill SmithNoch keine Bewertungen
- Otto Van Delden and Robin SmithuisDokument11 SeitenOtto Van Delden and Robin SmithuisSheila AnisaNoch keine Bewertungen
- Aghiz 3Dokument12 SeitenAghiz 3nandaaa aprilNoch keine Bewertungen
- Pancreatic Adenocarcinoma ImagingDokument9 SeitenPancreatic Adenocarcinoma ImagingDinesh RamaswamyNoch keine Bewertungen
- Hilar Cholangiocarcinoma Diagnosed and Treated Early, in Prejaundice PhaseDokument4 SeitenHilar Cholangiocarcinoma Diagnosed and Treated Early, in Prejaundice PhasebbdddNoch keine Bewertungen
- Biliary Duct ImagingDokument7 SeitenBiliary Duct ImagingImam FahriNoch keine Bewertungen
- Periampullary Carcinoma - Surgical Treatment - NCBI Bookshelf PDFDokument4 SeitenPeriampullary Carcinoma - Surgical Treatment - NCBI Bookshelf PDFAsif.N.IqbalNoch keine Bewertungen
- Modern Imaging in Obstructive JaundiceDokument4 SeitenModern Imaging in Obstructive JaundicedanaogreanuNoch keine Bewertungen
- Multidetector Computed Tomography in Hepatobiliary Lesions.Dokument11 SeitenMultidetector Computed Tomography in Hepatobiliary Lesions.Faiz arslanNoch keine Bewertungen
- Malignant Liver Tumors Undergrad 6th Year Students SharaanDokument56 SeitenMalignant Liver Tumors Undergrad 6th Year Students SharaanMohamed AhmedNoch keine Bewertungen
- CH 7Dokument11 SeitenCH 7Mr.ZeddNoch keine Bewertungen
- Liver CancerDokument44 SeitenLiver CancerEjay Jacob Ricamara50% (2)
- Distal Cholangiocarcinoma (DCC) : Paxton V. Dickson, MD, Stephen W. Behrman, MDDokument57 SeitenDistal Cholangiocarcinoma (DCC) : Paxton V. Dickson, MD, Stephen W. Behrman, MDALberta YosheNoch keine Bewertungen
- HCC NewDokument2 SeitenHCC NewHaridev AnandNoch keine Bewertungen
- Ampullarycarcinoma 140827105523 Phpapp02Dokument14 SeitenAmpullarycarcinoma 140827105523 Phpapp02Ai NguyenNoch keine Bewertungen
- Radiological Diagnosis and Staging of Hilar CholangiocarcinomaDokument13 SeitenRadiological Diagnosis and Staging of Hilar CholangiocarcinomaRirit Yuliarti Taha IINoch keine Bewertungen
- Case Report Klatskin TumorDokument5 SeitenCase Report Klatskin TumorwadejackNoch keine Bewertungen
- Diagnosticimagingof Hepaticlesionsinadults: Ramit Lamba,, Ghaneh Fananazapir,, Michael T. Corwin,, Vijay P. KhatriDokument32 SeitenDiagnosticimagingof Hepaticlesionsinadults: Ramit Lamba,, Ghaneh Fananazapir,, Michael T. Corwin,, Vijay P. KhatrifranciscoreynaNoch keine Bewertungen
- Colorectal Ca (CRC) .: Malueth Abraham, MBCHB ViDokument36 SeitenColorectal Ca (CRC) .: Malueth Abraham, MBCHB ViMalueth AnguiNoch keine Bewertungen
- Choledochal Cyst: SymposiumDokument3 SeitenCholedochal Cyst: SymposiumRegi Anastasya MangiriNoch keine Bewertungen
- Colorectal CancerDokument7 SeitenColorectal Cancerjames garciaNoch keine Bewertungen
- Colorrectal CancerDokument24 SeitenColorrectal CancerEzequiel GarciaNoch keine Bewertungen
- Liver CancerDokument44 SeitenLiver CancerJoyce Ann CumlatNoch keine Bewertungen
- Weber 2015Dokument12 SeitenWeber 2015Nikos SerifisNoch keine Bewertungen
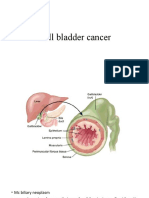
- Gall Bladder CancerDokument29 SeitenGall Bladder CancerJoju SebastianNoch keine Bewertungen
- Diagnosis and Treatment Update - CholangiocarcinomaDokument4 SeitenDiagnosis and Treatment Update - CholangiocarcinomaalfianfirdausNoch keine Bewertungen
- Biliary Cystadenocarcinoma With Mesenchymal Stroma: A Case ReportDokument7 SeitenBiliary Cystadenocarcinoma With Mesenchymal Stroma: A Case ReportAnalia RodriguezNoch keine Bewertungen
- Hepatocellular CarcinomaDokument9 SeitenHepatocellular CarcinomaGeorge WinchesterNoch keine Bewertungen
- Colorectal CancerDokument6 SeitenColorectal CancerAshiniNoch keine Bewertungen
- Autonomous VehiclesDokument11 SeitenAutonomous VehiclessoortaNoch keine Bewertungen
- Cholangiocarcinoma (Bile Duct Cancer)Dokument10 SeitenCholangiocarcinoma (Bile Duct Cancer)KibsJohnNoch keine Bewertungen
- Possible TreatmentsDokument1 SeitePossible Treatmentskuro hanabusaNoch keine Bewertungen
- Choledochal CystDokument3 SeitenCholedochal CystIqra FatemahNoch keine Bewertungen
- Liver Disease: Schwartz Principles of Surgery2010Dokument50 SeitenLiver Disease: Schwartz Principles of Surgery2010ralphNoch keine Bewertungen
- Wilm's Tumor RadiographyDokument8 SeitenWilm's Tumor RadiographyWowo Masthuro MahfudNoch keine Bewertungen
- Body ResearchDokument25 SeitenBody ResearchRoscelie KhoNoch keine Bewertungen
- Ca de Colon y Polipos PDFDokument24 SeitenCa de Colon y Polipos PDFGabriela Zavaleta CamachoNoch keine Bewertungen
- Fabrega 2016Dokument12 SeitenFabrega 2016Nikos SerifisNoch keine Bewertungen
- Acute and Chronic in Ammation of The Biliary SystemDokument4 SeitenAcute and Chronic in Ammation of The Biliary Systemfawzan mohammadNoch keine Bewertungen
- Benign Liver LesionsDokument30 SeitenBenign Liver LesionstheintrovNoch keine Bewertungen
- The Role of Imaging Methods in Identifying The Causes of Extrahepatic CholestasisDokument7 SeitenThe Role of Imaging Methods in Identifying The Causes of Extrahepatic CholestasisValian IndrianyNoch keine Bewertungen
- Common Bile Duct Stones StrictureDokument48 SeitenCommon Bile Duct Stones StrictureSyarif MalawatNoch keine Bewertungen
- Accuracy of Ultrasonography in The Diagnosis of Acute Calculous Cholecystitis: Review of The LiteratureDokument4 SeitenAccuracy of Ultrasonography in The Diagnosis of Acute Calculous Cholecystitis: Review of The LiteratureAnasriNstNoch keine Bewertungen
- Gastric Cancer by BalaDokument17 SeitenGastric Cancer by BalaArundeep AsaithambiNoch keine Bewertungen
- Liver CancerDokument12 SeitenLiver CancerPhạm Nguyễn Hoa HạNoch keine Bewertungen
- Carcinoma of Renal Pelvis and UreterDokument27 SeitenCarcinoma of Renal Pelvis and UreterIsaac MwangiNoch keine Bewertungen
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesVon EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNoch keine Bewertungen
- Gastrointestinal Endoscopy in the Cancer PatientVon EverandGastrointestinal Endoscopy in the Cancer PatientJohn C. DeutschNoch keine Bewertungen
- Falls: A Geriatric Syndrome: Jacqueline Jordan Lloyd, MD Florida State University College of MedicineDokument15 SeitenFalls: A Geriatric Syndrome: Jacqueline Jordan Lloyd, MD Florida State University College of MedicinePremaKurniaNoch keine Bewertungen
- Section 1. Definition and Classification of Acute Kidney InjuryDokument18 SeitenSection 1. Definition and Classification of Acute Kidney InjuryPremaKurniaNoch keine Bewertungen
- Roland Morris Low Back Pain and Disability Questionnaire rmq1 PDFDokument2 SeitenRoland Morris Low Back Pain and Disability Questionnaire rmq1 PDFPremaKurniaNoch keine Bewertungen
- Intravenous Fluid Therapy For Adults in Hospital Clinical GuidelineDokument10 SeitenIntravenous Fluid Therapy For Adults in Hospital Clinical GuidelinePremaKurniaNoch keine Bewertungen
- CHOLANGIOCARCINOMADokument26 SeitenCHOLANGIOCARCINOMAPremaKurnia100% (3)
- Use of White Blood Cell Count and Negative Appendectomy RateDokument8 SeitenUse of White Blood Cell Count and Negative Appendectomy RatePremaKurniaNoch keine Bewertungen
- Retinopathy of Prematurity Are Differentiated From Other Causes of Leukocoria. Most Important Differential Diagnosis IncludesDokument2 SeitenRetinopathy of Prematurity Are Differentiated From Other Causes of Leukocoria. Most Important Differential Diagnosis IncludesPremaKurniaNoch keine Bewertungen
- De Quervain S TenosynovitisDokument13 SeitenDe Quervain S TenosynovitisPremaKurniaNoch keine Bewertungen
- Osteomyelitis in Long Bones: by Luca Lazzarini, Jon T. Mader, and Jason H. CalhounDokument5 SeitenOsteomyelitis in Long Bones: by Luca Lazzarini, Jon T. Mader, and Jason H. CalhounPremaKurniaNoch keine Bewertungen
- Ticket Ticket: Medical FacultyDokument6 SeitenTicket Ticket: Medical Facultyhealer sruthyNoch keine Bewertungen
- Group 33 Module 7 ManuscriptDokument56 SeitenGroup 33 Module 7 ManuscriptMARIA KHIM ROSE BALCITANoch keine Bewertungen
- UNANG YAKAP (Essential Newborn Care Protocols)Dokument35 SeitenUNANG YAKAP (Essential Newborn Care Protocols)Jayson RN100% (1)
- Msds - AdditiveDokument9 SeitenMsds - AdditivedanalabNoch keine Bewertungen
- Behcet DiseaseDokument6 SeitenBehcet DiseasejbahalkehNoch keine Bewertungen
- PG DissertationDokument39 SeitenPG Dissertationavikalmanitripathi2023Noch keine Bewertungen
- Addiction Part 1 Benzodiazepines Side Effects, About Risk and AlternativesDokument11 SeitenAddiction Part 1 Benzodiazepines Side Effects, About Risk and AlternativesEga Candra FaurizaNoch keine Bewertungen
- HSE Commitment and Policy?Dokument6 SeitenHSE Commitment and Policy?radhesrikrishnaNoch keine Bewertungen
- Apixaban in Patients With Atrial FibrillationDokument12 SeitenApixaban in Patients With Atrial FibrillationthedancingseaNoch keine Bewertungen
- 3rd CRM ReportDokument163 Seiten3rd CRM ReportNational Child Health Resource Centre (NCHRC)Noch keine Bewertungen
- The Effects of Sleep Deprivation On Your BodyDokument21 SeitenThe Effects of Sleep Deprivation On Your BodyFaradilah Binti Ajma'inNoch keine Bewertungen
- Physical Education and Health 3 Grade 12 Module 3.docx 1Dokument19 SeitenPhysical Education and Health 3 Grade 12 Module 3.docx 1Iesha Rhaye Alonzo100% (2)
- A Last Resort?Dokument942 SeitenA Last Resort?SBS_NewsNoch keine Bewertungen
- Farmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiDokument19 SeitenFarmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiCici MastaNoch keine Bewertungen
- Mitchell H. Katz-Evaluating Clinical and Public Health Interventions - A Practical Guide To Study Design and Statistics (2010)Dokument176 SeitenMitchell H. Katz-Evaluating Clinical and Public Health Interventions - A Practical Guide To Study Design and Statistics (2010)Lakshmi SethNoch keine Bewertungen
- Sarcopenia, European Definition and DiagnosisDokument12 SeitenSarcopenia, European Definition and DiagnosisRémi DelauzunNoch keine Bewertungen
- Case 2 - The Global Biopharmaceutical IndustryDokument5 SeitenCase 2 - The Global Biopharmaceutical IndustryTran Bao DuongNoch keine Bewertungen
- The Factories Act 1948Dokument96 SeitenThe Factories Act 1948NIKITHAA ASHWINNoch keine Bewertungen
- 4th Year MBBS Batches & GroupsDokument2 Seiten4th Year MBBS Batches & GroupsSohail Abbas KhanNoch keine Bewertungen
- BrainHealthAssessment ReportDokument14 SeitenBrainHealthAssessment ReportJoe CohenNoch keine Bewertungen
- Full Psych DB InterviewDokument30 SeitenFull Psych DB InterviewAdam GNoch keine Bewertungen
- Tolin Et Al. - 2010 - Course of Compulsive Hoarding and Its RelationshipDokument11 SeitenTolin Et Al. - 2010 - Course of Compulsive Hoarding and Its RelationshipQon100% (1)
- Josh Fose Standards Web PDFDokument44 SeitenJosh Fose Standards Web PDFYasir QureshiNoch keine Bewertungen
- Acute Pancriatis Special HDokument9 SeitenAcute Pancriatis Special HInga CeagleiNoch keine Bewertungen
- Thomas Szasz On Freedom and Psychotherapy: Browse Articles & InterviewsDokument4 SeitenThomas Szasz On Freedom and Psychotherapy: Browse Articles & InterviewsGeorge RoseNoch keine Bewertungen
- History of Toxicity TestingDokument4 SeitenHistory of Toxicity TestingIja Nur100% (1)
- Treatment Aspects in Perioperative NursingDokument51 SeitenTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- Gynae Training ManualDokument30 SeitenGynae Training ManualKhushi Husna100% (1)