Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hasil Uji Validitas Dan ReliabilitasDokument7 SeitenHasil Uji Validitas Dan ReliabilitasNeniq SukutNoch keine Bewertungen
- Hasil Uji Regresi Linier Dengfan SpssDokument8 SeitenHasil Uji Regresi Linier Dengfan SpssNeniq SukutNoch keine Bewertungen
- Spil KitDokument1 SeiteSpil KitNeniq SukutNoch keine Bewertungen
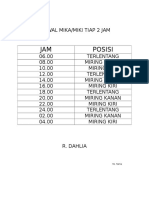
- Jadwal MikaDokument1 SeiteJadwal MikaNeniq SukutNoch keine Bewertungen
- Jadwal MikaDokument1 SeiteJadwal MikaNeniq SukutNoch keine Bewertungen
- Jadwal MikaDokument1 SeiteJadwal MikaNeniq SukutNoch keine Bewertungen
- Jadwal MikaDokument1 SeiteJadwal MikaNeniq SukutNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- DR Ahamad Hassan Stroke MimicsDokument23 SeitenDR Ahamad Hassan Stroke MimicskselvieNoch keine Bewertungen
- Integrative Behavioral Health Screening Tools and Resource ListDokument19 SeitenIntegrative Behavioral Health Screening Tools and Resource ListSkawnger SaluperNoch keine Bewertungen
- DESIGN AND DEVELOPMENT OF C-ARM MACHINE - Pptx.feem - Backup - 265248Dokument11 SeitenDESIGN AND DEVELOPMENT OF C-ARM MACHINE - Pptx.feem - Backup - 265248TamilandaNoch keine Bewertungen
- DPL OperationDokument2 SeitenDPL OperationTao JunNoch keine Bewertungen
- 2014 Final With Answers: 10000 SeriesDokument36 Seiten2014 Final With Answers: 10000 SeriesMareeswaranNoch keine Bewertungen
- Chronic Lymphocytic Leukemia/ Small Lymphocytic LymphomaDokument84 SeitenChronic Lymphocytic Leukemia/ Small Lymphocytic LymphomasimplyrosalynNoch keine Bewertungen
- Discharge PlanDokument1 SeiteDischarge PlanGail GenturalezNoch keine Bewertungen
- Gestational DiabetesDokument42 SeitenGestational Diabetesjohn jumborock100% (1)
- Past Psychiatric History ExamplesDokument11 SeitenPast Psychiatric History ExamplesEzra Denise Lubong RamelNoch keine Bewertungen
- Case Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisDokument26 SeitenCase Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisNatalia LoredanaNoch keine Bewertungen
- Record Below The Total Number of Cases and Deaths For Each Disease/condition For The Current WeekDokument2 SeitenRecord Below The Total Number of Cases and Deaths For Each Disease/condition For The Current WeekYohannes MengistNoch keine Bewertungen
- EREDokument3 SeitenERETin tinNoch keine Bewertungen
- Peritonsillar Abscess in Emergency MedicineDokument14 SeitenPeritonsillar Abscess in Emergency Medicinerissa neNoch keine Bewertungen
- Behavioral Pain Scale (BPS) For Pain Assessment in Intubated Patients - MDCalcDokument2 SeitenBehavioral Pain Scale (BPS) For Pain Assessment in Intubated Patients - MDCalcJeane SuyantoNoch keine Bewertungen
- Host ModulationDokument17 SeitenHost ModulationIbrar HumayunNoch keine Bewertungen
- Clinical Research As A CarreerDokument37 SeitenClinical Research As A Carreerrahil khanNoch keine Bewertungen
- AllianzDokument27 SeitenAllianzHariz SyahmiNoch keine Bewertungen
- Prepaid PlansDokument27 SeitenPrepaid PlansDee ReyesNoch keine Bewertungen
- Berberine and Weight LossDokument4 SeitenBerberine and Weight LossRoxana Frincu100% (1)
- Attachment 5 - Crew Health Declaration - 2015-09 - Ver0 (5) 2Dokument1 SeiteAttachment 5 - Crew Health Declaration - 2015-09 - Ver0 (5) 2Julessio SihombingNoch keine Bewertungen
- A Case Study On Severe MalariaDokument39 SeitenA Case Study On Severe Malariaokelue kingsleyNoch keine Bewertungen
- Clinical Questions PICO and Study Design EBM Part 1Dokument47 SeitenClinical Questions PICO and Study Design EBM Part 1Yaser ZaherNoch keine Bewertungen
- Oet PDFDokument8 SeitenOet PDFMary JisNoch keine Bewertungen
- Pendidikan Pasien Cath LabDokument10 SeitenPendidikan Pasien Cath LabAgnesthesiaNoch keine Bewertungen
- Immune Thrombocytopenia: Causes of Secondary ITPDokument3 SeitenImmune Thrombocytopenia: Causes of Secondary ITPkrataiwanNoch keine Bewertungen
- Pedia QDokument36 SeitenPedia QAmal100% (1)
- Ethical and Legal Issues in Reproductive HealthDokument4 SeitenEthical and Legal Issues in Reproductive HealthBianca_P0pNoch keine Bewertungen
- Urinalysis in Children and Adolescents, (2014)Dokument11 SeitenUrinalysis in Children and Adolescents, (2014)Enrique MANoch keine Bewertungen
- CICATRIX Pilot Study Final ReportDokument23 SeitenCICATRIX Pilot Study Final ReportKrish ShettyNoch keine Bewertungen
- Essay About Why We Need Physiology in Our LifeDokument8 SeitenEssay About Why We Need Physiology in Our LifeWendelieDescartinNoch keine Bewertungen