Das könnte Ihnen auch gefallen
- Fixed Orthodontic Appliances: A Practical GuideVon EverandFixed Orthodontic Appliances: A Practical GuideBewertung: 1 von 5 Sternen1/5 (1)
- Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsVon EverandSupra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsBewertung: 5 von 5 Sternen5/5 (1)
- Selecion of Major ConnectorsDokument2 SeitenSelecion of Major ConnectorsTanmay SrivastavaNoch keine Bewertungen
- The Complete Guide To Dentures: All About DentistryVon EverandThe Complete Guide To Dentures: All About DentistryNoch keine Bewertungen
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentVon EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNoch keine Bewertungen
- Fundamentals of Oral and Maxillofacial RadiologyVon EverandFundamentals of Oral and Maxillofacial RadiologyBewertung: 4 von 5 Sternen4/5 (1)
- Lecture 6 Acrylic RPDDokument23 SeitenLecture 6 Acrylic RPDAmmar AldawoodyehNoch keine Bewertungen
- Relining and Rebasing of Complete DenturesDokument28 SeitenRelining and Rebasing of Complete DenturesPurnama SyahbaniNoch keine Bewertungen
- Bds Tutorial Overdentures 1Dokument7 SeitenBds Tutorial Overdentures 1ikeuchi_ogawaNoch keine Bewertungen
- Biomechanics and Clinical Implications of Complete Edentulous StateDokument4 SeitenBiomechanics and Clinical Implications of Complete Edentulous StateDorobantuMihaiGabiNoch keine Bewertungen
- Dahl's ApplianceDokument7 SeitenDahl's AppliancerekabiNoch keine Bewertungen
- Jurnal DentistDokument8 SeitenJurnal DentistAnugrah AztriNoch keine Bewertungen
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethDokument11 SeitenOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcNoch keine Bewertungen
- Prostho Lec - OverdenturesDokument14 SeitenProstho Lec - Overdenturesdrgayen6042Noch keine Bewertungen
- Overdenture 4th Year 15-3-2020Dokument52 SeitenOverdenture 4th Year 15-3-2020Ahmed AliNoch keine Bewertungen
- Overdenture 140503222227 Phpapp01Dokument107 SeitenOverdenture 140503222227 Phpapp01TatsamYadavNoch keine Bewertungen
- Teeth Selection and ArrangementDokument118 SeitenTeeth Selection and Arrangementaakankshakanwar100% (2)
- Removable Partial DentureDokument16 SeitenRemovable Partial DentureRonald NarsicoNoch keine Bewertungen
- Cavitypreparation 130320103634 Phpapp01Dokument60 SeitenCavitypreparation 130320103634 Phpapp01Sumit BediNoch keine Bewertungen
- ISSN: 0975-833X: Research ArticleDokument9 SeitenISSN: 0975-833X: Research ArticleSuryo HannaNoch keine Bewertungen
- 12 Pin Retained RestorationDokument59 Seiten12 Pin Retained RestorationMohsin HabibNoch keine Bewertungen
- Basic Principles of Obturator Design IIDokument7 SeitenBasic Principles of Obturator Design IIGilberto Arturo Huapaya MarcosNoch keine Bewertungen
- My 3rd Seminar - DentinDokument25 SeitenMy 3rd Seminar - DentinJon YorkNoch keine Bewertungen
- Hand Out 2021 Restoration of Endodontically Treated TeethDokument40 SeitenHand Out 2021 Restoration of Endodontically Treated TeethpriyaNoch keine Bewertungen
- Removable Partial DentureDokument38 SeitenRemovable Partial DentureNissaNoch keine Bewertungen
- Management of Acquired Maxillary Defects Partially Edentlous PDFDokument129 SeitenManagement of Acquired Maxillary Defects Partially Edentlous PDFRamy Khalifa AshmawyNoch keine Bewertungen
- Direct RetainersDokument10 SeitenDirect RetainersSakinah SyahirahNoch keine Bewertungen
- Occlusal MoldsDokument7 SeitenOcclusal MoldsFrederico Diego Medeiros LimaNoch keine Bewertungen
- Complete Rehabilitation of A Patient With Occlusal Wear PDFDokument7 SeitenComplete Rehabilitation of A Patient With Occlusal Wear PDFsarfarazahmad19Noch keine Bewertungen
- Debate Acrylic Vs Cobalt ChromeDokument29 SeitenDebate Acrylic Vs Cobalt ChromeNafij JamayetNoch keine Bewertungen
- Single Complete DentureDokument23 SeitenSingle Complete DentureNelly SuriamahNoch keine Bewertungen
- Recent Advances in Provisional RestorationsDokument6 SeitenRecent Advances in Provisional RestorationsAngelia PratiwiNoch keine Bewertungen
- Direct Retainers (Infra Bulge)Dokument31 SeitenDirect Retainers (Infra Bulge)Bara Abdul0% (1)
- Partial Retainer in FPD DR VikasDokument99 SeitenPartial Retainer in FPD DR VikasVikas AggarwalNoch keine Bewertungen
- Complete Denture JourneyDokument30 SeitenComplete Denture JourneysapnaNoch keine Bewertungen
- 0 - A Clinical Guide To OcclusionDokument1 Seite0 - A Clinical Guide To Occlusionyhajo100% (1)
- Bicon Seating ChecklistDokument2 SeitenBicon Seating ChecklistRoger VergarayNoch keine Bewertungen
- Non Surgical Endodontic Retreatment: Presented byDokument58 SeitenNon Surgical Endodontic Retreatment: Presented bySayak GuptaNoch keine Bewertungen
- Occlusion / Orthodontic Courses by Indian Dental AcademyDokument90 SeitenOcclusion / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Balanced Occlu HandoutDokument9 SeitenBalanced Occlu HandoutMostafa FayadNoch keine Bewertungen
- Principles of Tooth PreparationDokument10 SeitenPrinciples of Tooth Preparationruchika100% (2)
- Intracoronal Attachments For Removable Partial DenturesDokument18 SeitenIntracoronal Attachments For Removable Partial Denturesapi-3710948100% (6)
- Practice: Restoration of The Root-Filled Tooth: Pre-Operative AssessmentDokument10 SeitenPractice: Restoration of The Root-Filled Tooth: Pre-Operative AssessmenteletiNoch keine Bewertungen
- Accurate ALginate ImpressionDokument2 SeitenAccurate ALginate Impressionlah_saneNoch keine Bewertungen
- Try in AppointmentDokument91 SeitenTry in Appointmentspu123Noch keine Bewertungen
- Surgical Extrusion: A Dental TechniqueDokument6 SeitenSurgical Extrusion: A Dental TechniqueDragos CiongaruNoch keine Bewertungen
- Preoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianDokument7 SeitenPreoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianS S Saad SaadNoch keine Bewertungen
- Alginate Impression MaterialDokument92 SeitenAlginate Impression MaterialrusschallengerNoch keine Bewertungen
- New Microsoft Office Word DocumentDokument3 SeitenNew Microsoft Office Word DocumentAtulsanapNoch keine Bewertungen
- Working Length DeterminationDokument97 SeitenWorking Length Determinationrolly_jatinNoch keine Bewertungen
- Congenitally Missing Maxillary Lateral IncisorsDokument56 SeitenCongenitally Missing Maxillary Lateral Incisorsdrsankhya100% (1)
- Relining and Rebasing of Complete DentureDokument7 SeitenRelining and Rebasing of Complete DentureAdinda YokoNoch keine Bewertungen
- RPD Clasp DesignDokument10 SeitenRPD Clasp DesignAmar BhochhibhoyaNoch keine Bewertungen
- Restoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghDokument100 SeitenRestoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghCahyani CahyaniNoch keine Bewertungen
- Infection Control in Fixed Prosthodontics: Prepared & Presented byDokument57 SeitenInfection Control in Fixed Prosthodontics: Prepared & Presented byaloooooooshNoch keine Bewertungen
- Failures in FPDDokument30 SeitenFailures in FPDMayank Aggarwal100% (1)
- Single Complete DenturesDokument20 SeitenSingle Complete DenturesDeepthi RajeshNoch keine Bewertungen
- Occlusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumDokument4 SeitenOcclusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumTung Thanh NguyenNoch keine Bewertungen
- ProsthoDokument59 SeitenProsthoramNoch keine Bewertungen
- QDWPlicDokument2 SeitenQDWPlicBibek RajNoch keine Bewertungen
- JdsmcxnksDokument32 SeitenJdsmcxnksBibek RajNoch keine Bewertungen
- For Mucocele Lesions - Careful Excisional BiopsyDokument11 SeitenFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNoch keine Bewertungen
- 3 UhnjkcDokument8 Seiten3 UhnjkcBibek RajNoch keine Bewertungen
- Curriculum Vitae: Personal DetailsDokument3 SeitenCurriculum Vitae: Personal DetailsBibek RajNoch keine Bewertungen
- Trapezoidal Flap. A Diagrammatic IllustrationDokument6 SeitenTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNoch keine Bewertungen
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDokument3 SeitenPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNoch keine Bewertungen
- When Is Oral Biopsy Not Needed?Dokument6 SeitenWhen Is Oral Biopsy Not Needed?Bibek RajNoch keine Bewertungen
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDokument73 SeitenInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNoch keine Bewertungen
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Dokument5 SeitenBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNoch keine Bewertungen
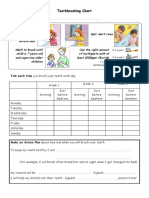
- Toothbrushing Chart PDFDokument1 SeiteToothbrushing Chart PDFBibek RajNoch keine Bewertungen
- Background Methods: Review' (OHAR) Guidance in BriefDokument1 SeiteBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNoch keine Bewertungen
- DhdifogkDokument4 SeitenDhdifogkBibek RajNoch keine Bewertungen
- JDJDJDJDokument23 SeitenJDJDJDJBibek RajNoch keine Bewertungen
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDokument1 SeiteBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNoch keine Bewertungen
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDokument6 SeitenVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNoch keine Bewertungen
- DrtfygbyuijDokument29 SeitenDrtfygbyuijBibek RajNoch keine Bewertungen
- YuybnunhhuhbDokument2 SeitenYuybnunhhuhbBibek RajNoch keine Bewertungen
- FfghhthjgvyujhDokument1 SeiteFfghhthjgvyujhBibek RajNoch keine Bewertungen
- YudsbhcjDokument1 SeiteYudsbhcjBibek RajNoch keine Bewertungen
- Dental Anxiety Form 4 PDFDokument2 SeitenDental Anxiety Form 4 PDFBibek RajNoch keine Bewertungen
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDokument2 SeitenUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNoch keine Bewertungen
- Rapid: Reducing Antibiotic Prescribing in DentistryDokument5 SeitenRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNoch keine Bewertungen
- Warfarin and Your Dental Treatment: Information For PatientsDokument5 SeitenWarfarin and Your Dental Treatment: Information For PatientsBibek RajNoch keine Bewertungen
- VfyggdbDokument33 SeitenVfyggdbBibek RajNoch keine Bewertungen
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDokument1 SeiteToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNoch keine Bewertungen
- TG 6 YhunjDokument48 SeitenTG 6 YhunjBibek RajNoch keine Bewertungen
- Pharma IndiaDokument58 SeitenPharma IndiaSaravana Kumar50% (4)
- NauliDokument2 SeitenNauliGurjit Singh BoparaiNoch keine Bewertungen
- Adhd Powerpoint-1Dokument21 SeitenAdhd Powerpoint-1api-516280936Noch keine Bewertungen
- Nurs 3021 Midterm Evaluation - Blessing Nwogu 1Dokument17 SeitenNurs 3021 Midterm Evaluation - Blessing Nwogu 1api-673227957Noch keine Bewertungen
- Indus Hospital - HR PDFDokument92 SeitenIndus Hospital - HR PDFdeva kiranNoch keine Bewertungen
- Sensors 22 08161 v2Dokument20 SeitenSensors 22 08161 v2Kristian DokicNoch keine Bewertungen
- Garden Trust Launches A CompetitionDokument3 SeitenGarden Trust Launches A CompetitionCami GrossiNoch keine Bewertungen
- Pepper PDFDokument52 SeitenPepper PDFMarie GregorioNoch keine Bewertungen
- California Retailers Guide To Hazardous Waste ComplianceDokument4 SeitenCalifornia Retailers Guide To Hazardous Waste ComplianceStericycle100% (1)
- Suggestive Questions of Isc 2023 BiologyDokument12 SeitenSuggestive Questions of Isc 2023 Biologyjahnvipatel2004Noch keine Bewertungen
- How Physical Activity Boosts Your Overall HealthDokument9 SeitenHow Physical Activity Boosts Your Overall HealthankiblogsNoch keine Bewertungen
- Infant Ventilator For Conventional Ventilation (Also Available With Optional HFO)Dokument8 SeitenInfant Ventilator For Conventional Ventilation (Also Available With Optional HFO)ROHIT KHANNANoch keine Bewertungen
- Clientele and Audiences in Social Work SEMIS DIASSDokument30 SeitenClientele and Audiences in Social Work SEMIS DIASSCharles CabarlesNoch keine Bewertungen
- 51 - Methemoglobin ProducersDokument20 Seiten51 - Methemoglobin ProducersCabinet VeterinarNoch keine Bewertungen
- IVT Network - Process Validation - 2014-04-28Dokument1 SeiteIVT Network - Process Validation - 2014-04-28Mina Maher MikhailNoch keine Bewertungen
- Health Concern in Computer Use PDFDokument23 SeitenHealth Concern in Computer Use PDFMicah Ellah Reynoso PatindolNoch keine Bewertungen
- Otda Foil Request 2Dokument4 SeitenOtda Foil Request 2sammyschwartz08Noch keine Bewertungen
- Chapter 16, Modern Advanced Accounting-Review Q & ExrDokument25 SeitenChapter 16, Modern Advanced Accounting-Review Q & Exrrlg4814100% (4)
- Emotional Intelligence in LEADERSDokument77 SeitenEmotional Intelligence in LEADERSImran MalikNoch keine Bewertungen
- Industrial Ergonomics SSRDokument35 SeitenIndustrial Ergonomics SSRShkar GalalyNoch keine Bewertungen
- Pengaruh Latihan Fisik Aerobik Dengan Intensitas Sedang Terhadap Kondisi Makroskopik Dan Gambaran Histopatologi Miokard Mencit Balb/CDokument8 SeitenPengaruh Latihan Fisik Aerobik Dengan Intensitas Sedang Terhadap Kondisi Makroskopik Dan Gambaran Histopatologi Miokard Mencit Balb/CBahar WahyuNoch keine Bewertungen
- TRAINING WORKSHOP FOR TRADITIONAL HERBAL MEDICAL PRACTIONERS Ode OmuDokument2 SeitenTRAINING WORKSHOP FOR TRADITIONAL HERBAL MEDICAL PRACTIONERS Ode OmuOlatunji Adebisi TundeNoch keine Bewertungen
- Provisional Mop Up Selection List For Neet PG CPS 2021Dokument47 SeitenProvisional Mop Up Selection List For Neet PG CPS 2021Rikesh K MhatreNoch keine Bewertungen
- Zero B Product PresentationDokument27 SeitenZero B Product PresentationKalyan DeshpandeNoch keine Bewertungen
- UAE Physiotherapy Organization FormationDokument1 SeiteUAE Physiotherapy Organization FormationDaniel Rivano-FischerNoch keine Bewertungen
- Mirena BrochureDokument24 SeitenMirena BrochureNamrata HarishNoch keine Bewertungen
- Review of Urban Drainage, 4th Edition, by David Butler, Christopher James Digman, Christos Makropoulos, and John W. DaviesDokument1 SeiteReview of Urban Drainage, 4th Edition, by David Butler, Christopher James Digman, Christos Makropoulos, and John W. DaviesJhon Edison Bravo Buitrago100% (1)
- 12life Saving RulesDokument33 Seiten12life Saving RulesLakshmi Kanth PNoch keine Bewertungen
- Social Responsibility of Business and Business Ethics: 2.1 IntroductionDokument25 SeitenSocial Responsibility of Business and Business Ethics: 2.1 IntroductionimadNoch keine Bewertungen
- Original PDF Kendigs Disorders of The Respiratory Tract in Children 9th Edition PDFDokument41 SeitenOriginal PDF Kendigs Disorders of The Respiratory Tract in Children 9th Edition PDFmichael.richardson540100% (30)