Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Unit 5-People Should Manage Nature-Ts-Planning Guide-Grade 5Dokument1 SeiteUnit 5-People Should Manage Nature-Ts-Planning Guide-Grade 5api-457240136Noch keine Bewertungen
- The Eclectic (OLI) Paradigm of International Production - Past, Present and FutureDokument19 SeitenThe Eclectic (OLI) Paradigm of International Production - Past, Present and FutureJomit C PNoch keine Bewertungen
- Microbial Agents of Obstetric and Gynecological InfectionsDokument70 SeitenMicrobial Agents of Obstetric and Gynecological InfectionsVilovand EtutNoch keine Bewertungen
- MWTCJF: Lion Air Eticket Itinerary / ReceiptDokument4 SeitenMWTCJF: Lion Air Eticket Itinerary / ReceiptVilovand EtutNoch keine Bewertungen
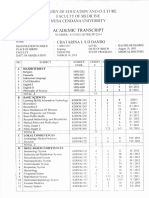
- Academic Transciript: Nusa Cendana UniviersiDokument1 SeiteAcademic Transciript: Nusa Cendana UniviersiVilovand EtutNoch keine Bewertungen
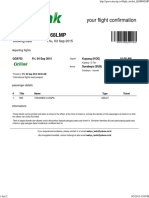
- H68LMP: Your Flight ConfirmationDokument4 SeitenH68LMP: Your Flight ConfirmationVilovand EtutNoch keine Bewertungen
- JeniDokument1 SeiteJeniVilovand EtutNoch keine Bewertungen
- Yblhxn: Lion Air Eticket Itinerary / ReceiptDokument2 SeitenYblhxn: Lion Air Eticket Itinerary / ReceiptVilovand EtutNoch keine Bewertungen
- GlobalisationDokument8 SeitenGlobalisationdummy12345Noch keine Bewertungen
- Fulltext PDFDokument454 SeitenFulltext PDFVirmantas JuoceviciusNoch keine Bewertungen
- AYURVEDA Products CatalogDokument17 SeitenAYURVEDA Products CatalogFoutanke TorodoNoch keine Bewertungen
- Pulsating Heat Pipe ReportDokument65 SeitenPulsating Heat Pipe ReportIdul Azharul HoqueNoch keine Bewertungen
- CH 11 International TradeDokument20 SeitenCH 11 International TradeSANTU GHORAINoch keine Bewertungen
- Iecex Bas 13.0069XDokument4 SeitenIecex Bas 13.0069XFrancesco_CNoch keine Bewertungen
- EVC AC Charger CatalogDokument2 SeitenEVC AC Charger CatalogRaison AutomationNoch keine Bewertungen
- Semi Formal Asking To Borrow BooksDokument75 SeitenSemi Formal Asking To Borrow BooksPei Cheng WuNoch keine Bewertungen
- Mindset For IELTS Level 1 Student's Book PDF English As A Second or Foreign Language International English Language TestinDokument1 SeiteMindset For IELTS Level 1 Student's Book PDF English As A Second or Foreign Language International English Language TestinhiNoch keine Bewertungen
- Quantum Data-Fitting: PACS Numbers: 03.67.-A, 03.67.ac, 42.50.DvDokument6 SeitenQuantum Data-Fitting: PACS Numbers: 03.67.-A, 03.67.ac, 42.50.Dvohenri100Noch keine Bewertungen
- Tescom Technical Training - Pressure Regulators Explained - Ver1.1Dokument19 SeitenTescom Technical Training - Pressure Regulators Explained - Ver1.1Amod DeshpandeNoch keine Bewertungen
- New DOCX DocumentDokument2 SeitenNew DOCX DocumentPunjabi FootballNoch keine Bewertungen
- Freeman Has Been A Partner in A Commercial Construction CompanyDokument1 SeiteFreeman Has Been A Partner in A Commercial Construction CompanyMuhammad ShahidNoch keine Bewertungen
- Learning Activity Sheet Pre-Calculus: Science Technology Engineering and Mathematics (STEM) Specialized SubjectDokument26 SeitenLearning Activity Sheet Pre-Calculus: Science Technology Engineering and Mathematics (STEM) Specialized SubjectJanet ComandanteNoch keine Bewertungen
- Bike LanesDokument12 SeitenBike LanesChitikala RajeshNoch keine Bewertungen
- Samsung WF8500NMW8Dokument180 SeitenSamsung WF8500NMW8Florin RusitoruNoch keine Bewertungen
- Vững vàng nền tảng, Khai sáng tương lai: Trang - 1Dokument11 SeitenVững vàng nền tảng, Khai sáng tương lai: Trang - 1An AnNoch keine Bewertungen
- Mrs. Saba Khan 15 Shahbad Diwan Khana, Bareilly, City, Bareilly, Bareilly, Utt AR PRADESH, 243003,9219172265Dokument28 SeitenMrs. Saba Khan 15 Shahbad Diwan Khana, Bareilly, City, Bareilly, Bareilly, Utt AR PRADESH, 243003,9219172265amitNoch keine Bewertungen
- Writing Capstone Research Project For Senior High School A Modified Guide ManualDokument9 SeitenWriting Capstone Research Project For Senior High School A Modified Guide ManualIOER International Multidisciplinary Research Journal ( IIMRJ)Noch keine Bewertungen
- Scriptcase MacrosDokument6 SeitenScriptcase MacrosMeliana WangNoch keine Bewertungen
- Radiology PearlsDokument2 SeitenRadiology PearlsSalman Rashid100% (2)
- Pipe Support Reference 8-29-14Dokument108 SeitenPipe Support Reference 8-29-14HITESHNoch keine Bewertungen
- Antibiotics and Their Types, Uses, Side EffectsDokument4 SeitenAntibiotics and Their Types, Uses, Side EffectsSpislgal PhilipNoch keine Bewertungen
- Simulado InglesDokument6 SeitenSimulado InglesWandercleyson da SilvaNoch keine Bewertungen
- Conformational AnalysisDokument4 SeitenConformational AnalysisJinNoch keine Bewertungen
- Republic V Mangotara DigestDokument3 SeitenRepublic V Mangotara DigestMickey Ortega100% (1)
- Amended August 8 2016Dokument31 SeitenAmended August 8 2016lux186Noch keine Bewertungen
- Resume Of: Name: Kingshuk Saha Address: Mobile: E-MailDokument2 SeitenResume Of: Name: Kingshuk Saha Address: Mobile: E-MailKingshuk Saha PalasNoch keine Bewertungen