Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Curriculum Vitae: Personal DetailsDokument3 SeitenCurriculum Vitae: Personal DetailsBibek RajNoch keine Bewertungen
- 3 UhnjkcDokument8 Seiten3 UhnjkcBibek RajNoch keine Bewertungen
- QDWPlicDokument2 SeitenQDWPlicBibek RajNoch keine Bewertungen
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Dokument5 SeitenBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNoch keine Bewertungen
- For Mucocele Lesions - Careful Excisional BiopsyDokument11 SeitenFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNoch keine Bewertungen
- JdsmcxnksDokument32 SeitenJdsmcxnksBibek RajNoch keine Bewertungen
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDokument73 SeitenInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNoch keine Bewertungen
- DhdifogkDokument4 SeitenDhdifogkBibek RajNoch keine Bewertungen
- Trapezoidal Flap. A Diagrammatic IllustrationDokument6 SeitenTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNoch keine Bewertungen
- When Is Oral Biopsy Not Needed?Dokument6 SeitenWhen Is Oral Biopsy Not Needed?Bibek RajNoch keine Bewertungen
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDokument3 SeitenPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNoch keine Bewertungen
- JDJDJDJDokument23 SeitenJDJDJDJBibek RajNoch keine Bewertungen
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDokument2 SeitenUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNoch keine Bewertungen
- YudsbhcjDokument1 SeiteYudsbhcjBibek RajNoch keine Bewertungen
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDokument6 SeitenVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNoch keine Bewertungen
- DrtfygbyuijDokument29 SeitenDrtfygbyuijBibek RajNoch keine Bewertungen
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDokument1 SeiteBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNoch keine Bewertungen
- YuybnunhhuhbDokument2 SeitenYuybnunhhuhbBibek RajNoch keine Bewertungen
- Background Methods: Review' (OHAR) Guidance in BriefDokument1 SeiteBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNoch keine Bewertungen
- FfghhthjgvyujhDokument1 SeiteFfghhthjgvyujhBibek RajNoch keine Bewertungen
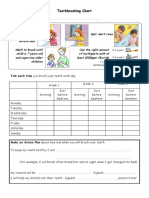
- Toothbrushing Chart PDFDokument1 SeiteToothbrushing Chart PDFBibek RajNoch keine Bewertungen
- Dental Anxiety Form 4 PDFDokument2 SeitenDental Anxiety Form 4 PDFBibek RajNoch keine Bewertungen
- Warfarin and Your Dental Treatment: Information For PatientsDokument5 SeitenWarfarin and Your Dental Treatment: Information For PatientsBibek RajNoch keine Bewertungen
- TG 6 YhunjDokument48 SeitenTG 6 YhunjBibek RajNoch keine Bewertungen
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDokument1 SeiteToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNoch keine Bewertungen
- Rapid: Reducing Antibiotic Prescribing in DentistryDokument5 SeitenRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNoch keine Bewertungen
- VfyggdbDokument33 SeitenVfyggdbBibek RajNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- UHV 2 MID 1 - Question BankDokument1 SeiteUHV 2 MID 1 - Question BankChaitanya SeesalaNoch keine Bewertungen
- BCE07Dokument18 SeitenBCE07jellaganeshNoch keine Bewertungen
- ORDEV Report On Employee ProactivityDokument24 SeitenORDEV Report On Employee ProactivityMary Pauline MuscaNoch keine Bewertungen
- Social Media On SocietyDokument2 SeitenSocial Media On SocietyNinggen HoomanNoch keine Bewertungen
- Andy Roxburgh - The Roll of Coach On The 21st Century - 2007 - FinlandDokument25 SeitenAndy Roxburgh - The Roll of Coach On The 21st Century - 2007 - FinlandDr. Victor StanculescuNoch keine Bewertungen
- Focus SystemDokument10 SeitenFocus SystemHarthwell CapistranoNoch keine Bewertungen
- How To RaidenDokument1 SeiteHow To Raidenhii hiiNoch keine Bewertungen
- Free Perfect Slave MoviesDokument4 SeitenFree Perfect Slave MovieslinnwotringNoch keine Bewertungen
- Reconcilable Differences? Standards-Based Teaching and DifferentiationDokument7 SeitenReconcilable Differences? Standards-Based Teaching and DifferentiationMohd Dzaquan ImranNoch keine Bewertungen
- The Awakened WarriorDokument11 SeitenThe Awakened WarriorGregg Swanson0% (1)
- Constituents and Categories of MethodsDokument7 SeitenConstituents and Categories of MethodsJohana Puerres NarváezNoch keine Bewertungen
- Crisis Management PlanDokument2 SeitenCrisis Management Planpoo12122100% (1)
- Organizational Behavior Midterm ExamDokument2 SeitenOrganizational Behavior Midterm ExamJove Roshanto NjotoamodjoNoch keine Bewertungen
- Chapter 1Dokument79 SeitenChapter 1CharleneKronstedt100% (1)
- 03252-6 Universal ThemesDokument2 Seiten03252-6 Universal ThemesThomas S. SpringerNoch keine Bewertungen
- Test Child Development and Pedagogy MCQS: Engineer Mushtaque Ahmed Rahu 1Dokument4 SeitenTest Child Development and Pedagogy MCQS: Engineer Mushtaque Ahmed Rahu 1Arbab Ali AbroNoch keine Bewertungen
- October 24 - Gestalt PsychologyDokument23 SeitenOctober 24 - Gestalt PsychologyEdgar Miralles Inales ManriquezNoch keine Bewertungen
- Compare, Contrast and Assess The Different Weaknesses of Deontology, Consequentialism and UtilitarianismDokument3 SeitenCompare, Contrast and Assess The Different Weaknesses of Deontology, Consequentialism and UtilitarianismAlondra L. FormenteraNoch keine Bewertungen
- The Old Man and The Sea: A Student Response Journal ForDokument6 SeitenThe Old Man and The Sea: A Student Response Journal ForMã Văn TàiNoch keine Bewertungen
- MODULE 1 - Art AppreciationDokument4 SeitenMODULE 1 - Art AppreciationMenard Jonas B. Mesoga75% (4)
- Factors Affecting Employee Motivation For Agri Vet Businesses Balandra 1Dokument123 SeitenFactors Affecting Employee Motivation For Agri Vet Businesses Balandra 1f.rickallen.balandraNoch keine Bewertungen
- CH 4 Notes Sensation and PerceptionDokument99 SeitenCH 4 Notes Sensation and Perceptionapi-261300427Noch keine Bewertungen
- The Borderline Personality by Elvis ObokDokument3 SeitenThe Borderline Personality by Elvis ObokOBOKNoch keine Bewertungen
- Johari WindowDokument1 SeiteJohari WindowPrashastiNoch keine Bewertungen
- Book On AutismDokument1 SeiteBook On AutismAbd ALRahmanNoch keine Bewertungen
- Men Take More 'Idiotic Risks,' Study Finds: Darwin AwardDokument2 SeitenMen Take More 'Idiotic Risks,' Study Finds: Darwin AwardGoranM.MuhammadNoch keine Bewertungen
- HG DLLDokument7 SeitenHG DLLFerdinand James PascuaNoch keine Bewertungen
- Language Training For Mining EngineersDokument6 SeitenLanguage Training For Mining Engineerscarhuazrca9226Noch keine Bewertungen
- Twig Journal Lesson PlanDokument5 SeitenTwig Journal Lesson Planapi-490399337Noch keine Bewertungen
- Week 4 Body LanguageDokument21 SeitenWeek 4 Body LanguageFadiah Nadhilah IrhadNoch keine Bewertungen