Das könnte Ihnen auch gefallen
- A Handbook of Hajj and UmrahDokument89 SeitenA Handbook of Hajj and UmrahUzaima SiddiquiNoch keine Bewertungen
- Rites of Hajj and Umrah by Sheikh Muhammad Nasiruddin Al-AlbaniDokument23 SeitenRites of Hajj and Umrah by Sheikh Muhammad Nasiruddin Al-AlbaniMuhammad ZameerNoch keine Bewertungen
- Activity Proposal Form: Proposed Date: Proposed TimeDokument2 SeitenActivity Proposal Form: Proposed Date: Proposed Timedrfaruqui2551Noch keine Bewertungen
- Bacillus Clausii As A Treatment of Small Intestinal Bacterial OvergrowthDokument2 SeitenBacillus Clausii As A Treatment of Small Intestinal Bacterial Overgrowthdrfaruqui2551Noch keine Bewertungen
- Efficacy of Bacillus Probiotics in Prevention of Antibiotic-Associated Diarrhoea: A Randomized, Double-Blind, Placebo-Controlled Clinical TrialDokument6 SeitenEfficacy of Bacillus Probiotics in Prevention of Antibiotic-Associated Diarrhoea: A Randomized, Double-Blind, Placebo-Controlled Clinical Trialdrfaruqui2551Noch keine Bewertungen
- Haj SummaryDokument16 SeitenHaj Summarydrfaruqui2551Noch keine Bewertungen
- Female Embryology, Anatomy and HistologyDokument43 SeitenFemale Embryology, Anatomy and Histologydrfaruqui2551Noch keine Bewertungen
- 27 Times Better Topical Versus OralDokument9 Seiten27 Times Better Topical Versus Oraldrfaruqui2551Noch keine Bewertungen
- ADR Form PDF File PDFDokument2 SeitenADR Form PDF File PDFdrfaruqui2551Noch keine Bewertungen
- 5GM BD For IbsDokument8 Seiten5GM BD For Ibsdrfaruqui2551Noch keine Bewertungen
- Dosages For ChildrenDokument1 SeiteDosages For Childrendrfaruqui2551Noch keine Bewertungen
- Aceclofenac A Reappraisal of Its Use in The.12Dokument30 SeitenAceclofenac A Reappraisal of Its Use in The.12drfaruqui2551Noch keine Bewertungen
- Coto StudyDokument8 SeitenCoto Studydrfaruqui2551Noch keine Bewertungen
- Curcumin and Chronic InflammationDokument32 SeitenCurcumin and Chronic Inflammationdrfaruqui2551Noch keine Bewertungen
- Visual-Procedural Memory Consolidation During Sleep Blocked by Glutamatergic Receptor AntagonistsDokument6 SeitenVisual-Procedural Memory Consolidation During Sleep Blocked by Glutamatergic Receptor Antagonistsdrfaruqui2551Noch keine Bewertungen
- Bacterial VaginosisDokument3 SeitenBacterial Vaginosisdrfaruqui2551Noch keine Bewertungen
- What Is DiabetesDokument2 SeitenWhat Is Diabetesdrfaruqui2551Noch keine Bewertungen
- Screening For DiabetesDokument2 SeitenScreening For Diabetesdrfaruqui2551Noch keine Bewertungen
- Antenatal CareDokument4 SeitenAntenatal Caredrfaruqui2551100% (1)
- CPHI2011Dokument2 SeitenCPHI2011drfaruqui2551Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Rwamagana s5 Mathematics CoreDokument4 SeitenRwamagana s5 Mathematics Coreevariste.ndungutse1493Noch keine Bewertungen
- Beng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtDokument9 SeitenBeng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtMarcelo BaptistaNoch keine Bewertungen
- FM Testbank-Ch18Dokument9 SeitenFM Testbank-Ch18David LarryNoch keine Bewertungen
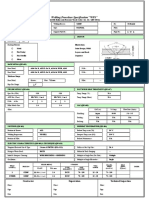
- Wps For Carbon Steel THK 7.11 GtawDokument1 SeiteWps For Carbon Steel THK 7.11 GtawAli MoosaviNoch keine Bewertungen
- The Impact of Personnel Behaviour in Clean RoomDokument59 SeitenThe Impact of Personnel Behaviour in Clean Roomisrael afolayan mayomiNoch keine Bewertungen
- DLL in Health 7 3rd QuarterDokument2 SeitenDLL in Health 7 3rd QuarterJuna Lyn Hermida ArellonNoch keine Bewertungen
- Note Hand-Soldering eDokument8 SeitenNote Hand-Soldering emicpreampNoch keine Bewertungen
- Retailing PPT (Shailwi Nitish)Dokument14 SeitenRetailing PPT (Shailwi Nitish)vinit PatidarNoch keine Bewertungen
- Papalia Welcome Asl 1 Guidelines 1 1Dokument14 SeitenPapalia Welcome Asl 1 Guidelines 1 1api-403316973Noch keine Bewertungen
- Lugam Annex Elementary School Second Quarter Second Periodical Test in EPP 6 H.EDokument4 SeitenLugam Annex Elementary School Second Quarter Second Periodical Test in EPP 6 H.Ejess amielNoch keine Bewertungen
- Vertical Cutoff WallsDokument18 SeitenVertical Cutoff WallsMark LaiNoch keine Bewertungen
- Assignment & Case Marketing Week 1: Max Van Neerven: 1664172 Mounir Trabelsi: 1705839 Renaldas Zlatkus: 1701775Dokument8 SeitenAssignment & Case Marketing Week 1: Max Van Neerven: 1664172 Mounir Trabelsi: 1705839 Renaldas Zlatkus: 1701775Ren ZkNoch keine Bewertungen
- ProjectDokument22 SeitenProjectSayan MondalNoch keine Bewertungen
- Oral Com Reviewer 1ST QuarterDokument10 SeitenOral Com Reviewer 1ST QuarterRaian PaderesuNoch keine Bewertungen
- Company Registration Procedure Handbook in Cambodia, EnglishDokument124 SeitenCompany Registration Procedure Handbook in Cambodia, EnglishThea100% (16)
- Turnbull CV OnlineDokument7 SeitenTurnbull CV Onlineapi-294951257Noch keine Bewertungen
- University of Southern Philippines Foundation. College of Engineering and ArchitectureDokument7 SeitenUniversity of Southern Philippines Foundation. College of Engineering and ArchitectureJason OwiaNoch keine Bewertungen
- Dash8 200 300 Electrical PDFDokument35 SeitenDash8 200 300 Electrical PDFCarina Ramo LakaNoch keine Bewertungen
- Assesment Test in English 9Dokument3 SeitenAssesment Test in English 9Chazz SatoNoch keine Bewertungen
- Thompson, Damon - Create A Servitor - How To Create A Servitor and Use The Power of Thought FormsDokument49 SeitenThompson, Damon - Create A Servitor - How To Create A Servitor and Use The Power of Thought FormsMike Cedersköld100% (5)
- Alienation Thesis StatementDokument8 SeitenAlienation Thesis Statementafbteepof100% (2)
- WeldingDokument23 SeitenWeldingMathan EverNoch keine Bewertungen
- Bobcat E34 - E35Z Brochure - Adare MachineryDokument8 SeitenBobcat E34 - E35Z Brochure - Adare MachineryNERDZONE TVNoch keine Bewertungen
- Annex A - Scope of WorkDokument4 SeitenAnnex A - Scope of Workمهيب سعيد الشميريNoch keine Bewertungen
- S P99 41000099DisplayVendorListDokument31 SeitenS P99 41000099DisplayVendorListMazen Sanad100% (1)
- Weekly Lesson Plan: Pry 3 (8years) Third Term Week 1Dokument12 SeitenWeekly Lesson Plan: Pry 3 (8years) Third Term Week 1Kunbi Santos-ArinzeNoch keine Bewertungen
- TRAVEL POLICY CARLO URRIZA OLIVAR Standard Insurance Co. Inc - Travel Protect - Print CertificateDokument4 SeitenTRAVEL POLICY CARLO URRIZA OLIVAR Standard Insurance Co. Inc - Travel Protect - Print CertificateCarlo OlivarNoch keine Bewertungen
- Ericsson For Sale From Powerstorm 4SA03071242Dokument8 SeitenEricsson For Sale From Powerstorm 4SA03071242wd3esaNoch keine Bewertungen
- Under Suitable Conditions, Butane, C: © OCR 2022. You May Photocopy ThisDokument13 SeitenUnder Suitable Conditions, Butane, C: © OCR 2022. You May Photocopy ThisMahmud RahmanNoch keine Bewertungen
- Sweat Equity SharesDokument8 SeitenSweat Equity SharesPratik RankaNoch keine Bewertungen