Das könnte Ihnen auch gefallen
- Research PCM 4 Group 2Dokument23 SeitenResearch PCM 4 Group 2Busay VelosoNoch keine Bewertungen
- DOH School Vaccination Program Provides Lifetime ImmunityDokument28 SeitenDOH School Vaccination Program Provides Lifetime ImmunityDarell Paguel Permato70% (10)
- Doh ProgramsDokument246 SeitenDoh ProgramsShengxy FerrerNoch keine Bewertungen
- Level of Awareness of Filipino Citizens Towards COVID-19Dokument62 SeitenLevel of Awareness of Filipino Citizens Towards COVID-19Nur Jehad MonirNoch keine Bewertungen
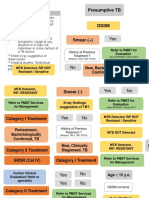
- Flowchart TB DOTSDokument11 SeitenFlowchart TB DOTSalfredtan6288Noch keine Bewertungen
- Saturday Group - Level of Knowledge On HIV AIDS Among Adolescents in Selected Barangays in Malapatan - LatestDokument77 SeitenSaturday Group - Level of Knowledge On HIV AIDS Among Adolescents in Selected Barangays in Malapatan - Latestromie_galloNoch keine Bewertungen
- Factors Affecting COVID-19 Vaccine Hesitancy Among Senior High Schools StudentsDokument18 SeitenFactors Affecting COVID-19 Vaccine Hesitancy Among Senior High Schools StudentsNicko TabanaoNoch keine Bewertungen
- Republic of The Philippines Pablo Borbon Main II Batangas CityDokument75 SeitenRepublic of The Philippines Pablo Borbon Main II Batangas CityklareNoch keine Bewertungen
- Covid-19 Vaccination Hesitancy A ReviewDokument4 SeitenCovid-19 Vaccination Hesitancy A ReviewInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Empowering Young Filipinos with Adolescent HealthDokument54 SeitenEmpowering Young Filipinos with Adolescent HealthChing Bocanegra AmorNoch keine Bewertungen
- Hiv/AidsDokument32 SeitenHiv/AidsFred C. MirandaNoch keine Bewertungen
- ESR Verification Form - Dec2015Dokument2 SeitenESR Verification Form - Dec2015Sandro Redoble100% (2)
- Ethico-Legal Considerations in The Care of Older AdultDokument25 SeitenEthico-Legal Considerations in The Care of Older AdultMarlone James OcenaNoch keine Bewertungen
- Region V leads in peritoneal dialysis uptakeDokument36 SeitenRegion V leads in peritoneal dialysis uptakeDaNiel AUreusNoch keine Bewertungen
- Community Diagnosis FPT - Chapter 1Dokument19 SeitenCommunity Diagnosis FPT - Chapter 1Katherine 'Chingboo' Leonico Laud100% (1)
- Fatima 121 ThesisDokument144 SeitenFatima 121 ThesisNecesario BanaagNoch keine Bewertungen
- Effects of Global Warming On Our HealthDokument3 SeitenEffects of Global Warming On Our HealthRifat Rahman SiumNoch keine Bewertungen
- Health Care Delivery System Lecture Handout PDFDokument9 SeitenHealth Care Delivery System Lecture Handout PDFelle bello100% (1)
- Typhoid Fever: Infectious DiseaseDokument52 SeitenTyphoid Fever: Infectious Disease12. Akshit AtwalNoch keine Bewertungen
- Unequal Distribution of Health Services Biggest Global Health ProblemDokument3 SeitenUnequal Distribution of Health Services Biggest Global Health ProblemHaleemaMunir0% (1)
- Hiv-Sle Case StudyDokument8 SeitenHiv-Sle Case StudycathyNoch keine Bewertungen
- Pregnancy Knowledge, Attitudes, and Practices inDokument210 SeitenPregnancy Knowledge, Attitudes, and Practices inazida90Noch keine Bewertungen
- Primary Health Care Maternal & Child HealthDokument32 SeitenPrimary Health Care Maternal & Child HealthAbidah Rahmi HilmyNoch keine Bewertungen
- Epidemiology and the Nurse: Understanding Disease Causation and Community ReactionsDokument70 SeitenEpidemiology and the Nurse: Understanding Disease Causation and Community ReactionsFilipina EpistolarianNoch keine Bewertungen
- Philippine College of Health Science IncDokument23 SeitenPhilippine College of Health Science Incpeter bruceNoch keine Bewertungen
- FPCBT Level 1 For FacilitatorsDokument519 SeitenFPCBT Level 1 For FacilitatorsMichael Villavert100% (1)
- Healthy Young OnesDokument49 SeitenHealthy Young OnesMARIA KATRINA NUVAL100% (2)
- Immunization Knowledge, Attitudes and PracticesDokument94 SeitenImmunization Knowledge, Attitudes and PracticesJohnrey Tesoro100% (5)
- Doh Hiv Art RegistryDokument7 SeitenDoh Hiv Art Registryrommel mendoza100% (1)
- COMMUNITY HEALTH PROFILE OF BARANGAY 142Dokument20 SeitenCOMMUNITY HEALTH PROFILE OF BARANGAY 142Helen Fairodz AmoraNoch keine Bewertungen
- HIV AwarenessDokument39 SeitenHIV AwarenessAlexCorchNoch keine Bewertungen
- Community Assessment Windshield Survey - EditedDokument8 SeitenCommunity Assessment Windshield Survey - EditedGeorge OwuorNoch keine Bewertungen
- Public Health Nursing 8X13Dokument11 SeitenPublic Health Nursing 8X13RUIZ JAKE CANCILLER. VELARDENoch keine Bewertungen
- Extent of Compliance and Perception of Mothers On Childhood Immunization in Barangay Ugac Sur, Tuguegarao City, Philippines: A Descriptive StudyDokument6 SeitenExtent of Compliance and Perception of Mothers On Childhood Immunization in Barangay Ugac Sur, Tuguegarao City, Philippines: A Descriptive StudyMamta AgarwalNoch keine Bewertungen
- MAN Thesis JonaberTM PDFDokument139 SeitenMAN Thesis JonaberTM PDFNashimah Bint Langilao-SYuken LHendersonNoch keine Bewertungen
- Understanding the Complex Factors Driving Vaccine Hesitancy in 40 CharactersDokument6 SeitenUnderstanding the Complex Factors Driving Vaccine Hesitancy in 40 CharactersAlexandra Mae D. MiguelNoch keine Bewertungen
- DENGUE PREVENTION AND CONTROL PROGRAMDokument7 SeitenDENGUE PREVENTION AND CONTROL PROGRAMFatima Grace EchemNoch keine Bewertungen
- PCV13 Vaccine Orientation for Misamis Oriental and Nearby ProvincesDokument24 SeitenPCV13 Vaccine Orientation for Misamis Oriental and Nearby ProvincesJay AdamzNoch keine Bewertungen
- CO ContentDokument312 SeitenCO ContentJonas Dela Cruz100% (1)
- Buntis Congress 2021 GiveawaysDokument24 SeitenBuntis Congress 2021 GiveawaysGiselle ArenasNoch keine Bewertungen
- Implications of HIV and AIDSDokument17 SeitenImplications of HIV and AIDSfarah_hhrrNoch keine Bewertungen
- DengueDokument5 SeitenDengueSam Angelo EstrellaNoch keine Bewertungen
- Prevention of Nosocomial Infections As Percieved by Staff Nurses - For SubmisionDokument31 SeitenPrevention of Nosocomial Infections As Percieved by Staff Nurses - For SubmisionDhonnalyn Amene CaballeroNoch keine Bewertungen
- Parental Decision Making On Childhood Vaccine - Final PaperDokument105 SeitenParental Decision Making On Childhood Vaccine - Final PaperOH WELL100% (1)
- The National Hiv and Aids Registry Manual of OperationsDokument136 SeitenThe National Hiv and Aids Registry Manual of OperationsPaulSimonNamocDivino50% (2)
- Special Health Concerns: C. Disaster Risk Reduction ManagementDokument8 SeitenSpecial Health Concerns: C. Disaster Risk Reduction ManagementWilma BeraldeNoch keine Bewertungen
- Review of Related LiteratureDokument11 SeitenReview of Related LiteratureJenniferAnneAlegre100% (1)
- Effects of Family Planning Units On The People of Ijebu-Ode, Ogun State, NigeriaDokument63 SeitenEffects of Family Planning Units On The People of Ijebu-Ode, Ogun State, NigeriaAderibigbe Adesoji DavidNoch keine Bewertungen
- Vanguards of Duty Exploring The Lived Experiences of Healthcare Frontliners During Pandemic SurgeDokument15 SeitenVanguards of Duty Exploring The Lived Experiences of Healthcare Frontliners During Pandemic SurgeInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- RESEARCH093016Dokument28 SeitenRESEARCH093016Satra Sabbuh100% (1)
- Diabetes DOH ProgramDokument14 SeitenDiabetes DOH ProgramJason MirasolNoch keine Bewertungen
- The Level of Awareness of ParentsDokument40 SeitenThe Level of Awareness of ParentsKevin Mark Marcelo Garcillan100% (1)
- Understanding STI/HIV and their PreventionDokument89 SeitenUnderstanding STI/HIV and their Preventionpedrong dodongNoch keine Bewertungen
- Integrating Severe Acute Malnutrition Into The Management of Childhood Diseases at Community Level in South SudanDokument36 SeitenIntegrating Severe Acute Malnutrition Into The Management of Childhood Diseases at Community Level in South Sudanmalaria_consortium100% (1)
- in Non-Communicable Diseases PART 1Dokument15 Seitenin Non-Communicable Diseases PART 1Deanne AbadNoch keine Bewertungen
- Breastfeeding HospitalDokument37 SeitenBreastfeeding Hospitalemmanjabasa100% (1)
- Lourlyn's Angels?Dokument27 SeitenLourlyn's Angels?lovelove DayoNoch keine Bewertungen
- Community Health Needs Assessment GuidelinesDokument22 SeitenCommunity Health Needs Assessment Guidelinesnailawe100% (2)
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutVon EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutBewertung: 5 von 5 Sternen5/5 (1)
- City Hall PrayerDokument1 SeiteCity Hall PrayerFritz MaandigNoch keine Bewertungen
- Iran-US Negotiation AnalysisDokument4 SeitenIran-US Negotiation AnalysisFritz MaandigNoch keine Bewertungen
- Gad 2017 AccomplishmentDokument7 SeitenGad 2017 AccomplishmentFritz MaandigNoch keine Bewertungen
- 2014 AIDS Epidemic Model - Impact Modeling and AnalysisDokument108 Seiten2014 AIDS Epidemic Model - Impact Modeling and AnalysisFritz MaandigNoch keine Bewertungen
- Conflict of Laws Notes - Agpalo Book PDFDokument40 SeitenConflict of Laws Notes - Agpalo Book PDFblueberry712100% (19)
- Action 1Dokument48 SeitenAction 1Fritz MaandigNoch keine Bewertungen
- Torts and Damages NotesDokument45 SeitenTorts and Damages NotesFritz Maandig100% (1)
- HandwritingDokument4 SeitenHandwritingartunianNoch keine Bewertungen
- Nachura Notes Local GovernmentsDokument34 SeitenNachura Notes Local GovernmentsNowhere Man100% (16)
- SC's Significant Decisions 2013-2015Dokument54 SeitenSC's Significant Decisions 2013-2015Fritz MaandigNoch keine Bewertungen
- What Are The Vulnerable Sectors in Philippine Society?Dokument4 SeitenWhat Are The Vulnerable Sectors in Philippine Society?Fritz MaandigNoch keine Bewertungen
- 2010 - 2015 - Income Tax PDFDokument31 Seiten2010 - 2015 - Income Tax PDFExequielCamisaCrusperoNoch keine Bewertungen
- College Board Recommended BooksDokument5 SeitenCollege Board Recommended BooksjamesbaquetNoch keine Bewertungen
- Demand Letter Sample PhillippinesDokument1 SeiteDemand Letter Sample PhillippinesMousy GamalloNoch keine Bewertungen
- FINALforsubmission Pedro JosefaDokument10 SeitenFINALforsubmission Pedro JosefaFritz MaandigNoch keine Bewertungen
- Republic Vs Sandigan (Ramas)Dokument25 SeitenRepublic Vs Sandigan (Ramas)Fritz MaandigNoch keine Bewertungen
- Arise People From Your SlumberDokument1 SeiteArise People From Your SlumberFritz MaandigNoch keine Bewertungen
- Article On ESA Drugs That Treat AnemiaDokument3 SeitenArticle On ESA Drugs That Treat AnemiaFritz MaandigNoch keine Bewertungen
- Weekly Calendar Landscape 5Dokument1 SeiteWeekly Calendar Landscape 5Duncan BusserNoch keine Bewertungen
- Nurses in Other Healthcare FieldDokument2 SeitenNurses in Other Healthcare FieldFritz MaandigNoch keine Bewertungen
- Full TextDokument281 SeitenFull TextAnđela AračićNoch keine Bewertungen
- Bora Study (Content)Dokument46 SeitenBora Study (Content)kasamahumanrightsNoch keine Bewertungen
- Case Study: Lindsey Vonn's Sports Illustrated CoverDokument7 SeitenCase Study: Lindsey Vonn's Sports Illustrated Coverapi-297929567Noch keine Bewertungen
- Transing Religious StudiesDokument17 SeitenTransing Religious StudiesDiegoNoch keine Bewertungen
- SampleDokument2 SeitenSampleapi-302832475Noch keine Bewertungen
- Test Bank For Reflect Relate An Introduction To Interpersonal Communication 5th Edition Steven Mccornack Kelly MorrisonDokument13 SeitenTest Bank For Reflect Relate An Introduction To Interpersonal Communication 5th Edition Steven Mccornack Kelly Morrisontintiedraweropw9100% (26)
- 2 - The Escalation LadderDokument26 Seiten2 - The Escalation LadderDan Mihai100% (4)
- CHAPTER 9 Robbery Investigation TechniquesDokument23 SeitenCHAPTER 9 Robbery Investigation Techniquesnicole rigonNoch keine Bewertungen
- Thank you for sharing this helpful information on incontinence. Let's move our discussion to identifying the patient and obtaining their historyDokument114 SeitenThank you for sharing this helpful information on incontinence. Let's move our discussion to identifying the patient and obtaining their historyManisanthosh Kumar88% (8)
- Human Immunodefficiency Syndrome: Nkelia Jones, Nikita JacobsDokument26 SeitenHuman Immunodefficiency Syndrome: Nkelia Jones, Nikita JacobsNikita JacobsNoch keine Bewertungen
- 7DO Day2Dokument17 Seiten7DO Day2Harjit Singh100% (1)
- 11.4 WorksheetDokument3 Seiten11.4 WorksheetJyoti SinghNoch keine Bewertungen
- Penny Genetics How Well Does A Punnett Square Predict The Actual RatiosDokument3 SeitenPenny Genetics How Well Does A Punnett Square Predict The Actual RatiosnataNoch keine Bewertungen
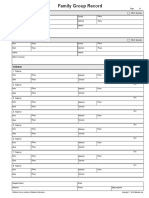
- FamilyGroupRecord PDFDokument1 SeiteFamilyGroupRecord PDFtereNoch keine Bewertungen
- FSFI Questionnaire Behind Addyi, The Female Sex PillDokument4 SeitenFSFI Questionnaire Behind Addyi, The Female Sex PillToronto StarNoch keine Bewertungen
- AHE Pro Human Environment TypedDokument52 SeitenAHE Pro Human Environment TypedK Praveen AryaNoch keine Bewertungen
- Ethical Decision Making nsg434Dokument6 SeitenEthical Decision Making nsg434api-470941612Noch keine Bewertungen
- Story Comm #129: "Offering To The Dawn"Dokument13 SeitenStory Comm #129: "Offering To The Dawn"Szymon SłomskiNoch keine Bewertungen
- Criminal Law Rape DefinitionDokument3 SeitenCriminal Law Rape DefinitionAkshay DhawanNoch keine Bewertungen
- Module 1 Name: Schedule: UNIT 1 Sex, Gender, and SexualityDokument15 SeitenModule 1 Name: Schedule: UNIT 1 Sex, Gender, and SexualityChan ChanNoch keine Bewertungen
- Literary Elements of 'ScheherazadeDokument3 SeitenLiterary Elements of 'ScheherazadeYhazmin Iris IlustrisimoNoch keine Bewertungen
- Vaginal SeptumDokument6 SeitenVaginal SeptumIntan Nuraini HakaNoch keine Bewertungen
- 0020 BASTI - Enema - Therapy - AS - ARDHA - CHIKITSA - A PDFDokument7 Seiten0020 BASTI - Enema - Therapy - AS - ARDHA - CHIKITSA - A PDFMSKCNoch keine Bewertungen
- Biological Factors in Human SexualityDokument8 SeitenBiological Factors in Human SexualityDevon ColeNoch keine Bewertungen
- KHC 4 Letting It All GoDokument21 SeitenKHC 4 Letting It All GojustnewaroundNoch keine Bewertungen
- TranslationDokument30 SeitenTranslationJohn Aries Almelor SarzaNoch keine Bewertungen
- Report On Family (Part 3)Dokument2 SeitenReport On Family (Part 3)Emmarlone96Noch keine Bewertungen
- 50 Facts About WomenDokument5 Seiten50 Facts About WomenAndrew AndersonNoch keine Bewertungen
- Vancouver References StyleDokument10 SeitenVancouver References StylePitambar PoudelNoch keine Bewertungen
- Expectations of Women in SocietyDokument11 SeitenExpectations of Women in Societyliliana cambasNoch keine Bewertungen