Das könnte Ihnen auch gefallen
- Clinical AnestesiaDokument432 SeitenClinical AnestesiaAde Putra100% (1)
- Medical Response to Child Sexual Abuse: A Resource for Professionals Working with Children and FamiliesVon EverandMedical Response to Child Sexual Abuse: A Resource for Professionals Working with Children and FamiliesNoch keine Bewertungen
- Paediatric & Adolescent GynaecologyDokument78 SeitenPaediatric & Adolescent GynaecologyMichelle FynesNoch keine Bewertungen
- Kuan Yin 100 Divine Lots InterpretationDokument30 SeitenKuan Yin 100 Divine Lots InterpretationEsperanza Theiss100% (2)
- Spleen/Liver Trauma DiagnosisDokument34 SeitenSpleen/Liver Trauma DiagnosissanjayNoch keine Bewertungen
- Medad Andrology Special Note NMT13 PDFDokument70 SeitenMedad Andrology Special Note NMT13 PDFSelim TarekNoch keine Bewertungen
- The Reproductive SystemDokument266 SeitenThe Reproductive SystemNatia DemetradzeNoch keine Bewertungen
- 2014 Pediatric & Adolescent GynecologyDokument77 Seiten2014 Pediatric & Adolescent GynecologyJai CarungayNoch keine Bewertungen
- Pediatric Gynecology Care & ExamsDokument70 SeitenPediatric Gynecology Care & ExamsBianca Denise FranciscoNoch keine Bewertungen
- El Bill PDFDokument2 SeitenEl Bill PDFvinodNoch keine Bewertungen
- Pap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.DDokument22 SeitenPap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.Dshygirl72Noch keine Bewertungen
- Hormonal ContraceptivesDokument25 SeitenHormonal Contraceptivesmd easarur rahmanNoch keine Bewertungen
- Infertility IDokument36 SeitenInfertility Idr_asaleh100% (1)
- Complications of Spinal and Epidural AnesthesiaDokument45 SeitenComplications of Spinal and Epidural AnesthesiashikhaNoch keine Bewertungen
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Dokument26 SeitenS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- Genital Anatomy in Non-Abused Preschool GirlsDokument10 SeitenGenital Anatomy in Non-Abused Preschool Girlsวินจนเซ ชินกิNoch keine Bewertungen
- Peugeot 206 Fuse Diagram PDFDokument6 SeitenPeugeot 206 Fuse Diagram PDFDedi dwi susanto100% (2)
- And Tab 1Dokument4 SeitenAnd Tab 1Bella SuratmonoNoch keine Bewertungen
- Physical Exam in Adolescent GynecologyDokument13 SeitenPhysical Exam in Adolescent GynecologyEric FatrinNoch keine Bewertungen
- Idiopathic Central Precocious Puberty A Case ReportDokument8 SeitenIdiopathic Central Precocious Puberty A Case ReportCarolyn CapisnonNoch keine Bewertungen
- Intermediate-Level Adolescent and Adult Sexual Assault Assessment: SANE/SAFE Forensic Learning SeriesVon EverandIntermediate-Level Adolescent and Adult Sexual Assault Assessment: SANE/SAFE Forensic Learning SeriesNoch keine Bewertungen
- Treatment and Outcomes of Precocious Puberty: An UpdateDokument11 SeitenTreatment and Outcomes of Precocious Puberty: An UpdateAbdurrahman Hasanuddin100% (1)
- Kegel Handout PDFDokument1 SeiteKegel Handout PDFMini ManojNoch keine Bewertungen
- Physical Findings in Child Sexual AbuseDokument14 SeitenPhysical Findings in Child Sexual AbusemeganitaNoch keine Bewertungen
- Identification and Management of Ambiguous GenitaliaDokument31 SeitenIdentification and Management of Ambiguous Genitaliateslimolakunleraji100% (1)
- Tall StatureDokument24 SeitenTall StaturedianmutiaNoch keine Bewertungen
- Medicolegal Issues in Obstetrics and Gynaecology: Swati Jha Emma FerrimanDokument374 SeitenMedicolegal Issues in Obstetrics and Gynaecology: Swati Jha Emma Ferrimankhalid balshaNoch keine Bewertungen
- Levin2004 Sexual Arousal PDFDokument7 SeitenLevin2004 Sexual Arousal PDFHenriqueSimãoNoch keine Bewertungen
- MCQ AnsDokument65 SeitenMCQ AnsFatima Hasnain100% (7)
- Growth & Development of An Adolescent (2380)Dokument8 SeitenGrowth & Development of An Adolescent (2380)ta CNoch keine Bewertungen
- Uterine FibroidsDokument21 SeitenUterine FibroidsPrasun BiswasNoch keine Bewertungen
- Puberty: Normal Development and Causes of Precocious PubertyDokument8 SeitenPuberty: Normal Development and Causes of Precocious Pubertyclear mindNoch keine Bewertungen
- The Use of Aromatase Inhibitors in Infertility and GynecologyDokument9 SeitenThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusNoch keine Bewertungen
- Puberty Normal and AbnormalDokument41 SeitenPuberty Normal and AbnormalTonyScariaNoch keine Bewertungen
- Movie Ethics ReviewDokument4 SeitenMovie Ethics ReviewpearlydawnNoch keine Bewertungen
- Physiology and PubertyDokument8 SeitenPhysiology and PubertynofiajahNoch keine Bewertungen
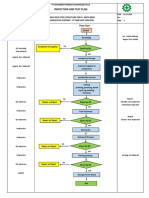
- Inspection and Test Plan: Flow Chart Start IncomingDokument1 SeiteInspection and Test Plan: Flow Chart Start IncomingSinden AyuNoch keine Bewertungen
- Reproductive EndocrinologyDokument18 SeitenReproductive EndocrinologyAnonymous hkWIKjoXFVNoch keine Bewertungen
- Anatomy and PhysiologyDokument8 SeitenAnatomy and PhysiologyAironne ManguilimotanNoch keine Bewertungen
- Diploma Pharmacy First Year - Hap - MCQSDokument13 SeitenDiploma Pharmacy First Year - Hap - MCQSAnitha Mary Dambale91% (33)
- Male InfertilityDokument57 SeitenMale InfertilityUsha AnengaNoch keine Bewertungen
- Conder Separator Brochure NewDokument8 SeitenConder Separator Brochure Newednavilod100% (1)
- Primary and Secondary AmenorrhoeaDokument72 SeitenPrimary and Secondary Amenorrhoead clarkeNoch keine Bewertungen
- Taking History and Physical Examination in YouthDokument99 SeitenTaking History and Physical Examination in Youthlinda ratna watiNoch keine Bewertungen
- Abnormal Development of Female Genital TractDokument69 SeitenAbnormal Development of Female Genital TractJerry CreedNoch keine Bewertungen
- Medical Findings and Child Sexual AbuseDokument26 SeitenMedical Findings and Child Sexual AbuseEdgar Aleman CruzNoch keine Bewertungen
- Genital examination findings - Understanding what is normalDokument36 SeitenGenital examination findings - Understanding what is normalMuhammad AuliaNoch keine Bewertungen
- Sexual Precocity PDFDokument5 SeitenSexual Precocity PDFmist73Noch keine Bewertungen
- 05 Skin AssessmentDokument31 Seiten05 Skin AssessmentHerlinaNababanNoch keine Bewertungen
- Precocious PubertyDokument30 SeitenPrecocious PubertyNeha SharmaNoch keine Bewertungen
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Dokument31 SeitenPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviNoch keine Bewertungen
- Precocious VS Early Puberty, SiskaDokument21 SeitenPrecocious VS Early Puberty, SiskapuspaNoch keine Bewertungen
- Congenital Anomelies of Reproductive OrgansDokument47 SeitenCongenital Anomelies of Reproductive Organsdr_shamimrNoch keine Bewertungen
- Management of Foreskin ConditionsDokument26 SeitenManagement of Foreskin ConditionsSarif CassanovaNoch keine Bewertungen
- Hypospadias Surgery: An Illustrated GuideVon EverandHypospadias Surgery: An Illustrated GuideAhmed HadidiBewertung: 5 von 5 Sternen5/5 (1)
- Kuliah Penis & ScrotumDokument13 SeitenKuliah Penis & ScrotumEmallia Phypiet FitrianiNoch keine Bewertungen
- Circumcision Using The Mogen ClampDokument4 SeitenCircumcision Using The Mogen ClampJorge AndrésNoch keine Bewertungen
- Anatomi PenisDokument1 SeiteAnatomi Penischouko catNoch keine Bewertungen
- Proper Circumcision Techniques for Infants and AdultsDokument6 SeitenProper Circumcision Techniques for Infants and Adultsntambik21Noch keine Bewertungen
- Congenital Malformations of The Female Genital TractDokument7 SeitenCongenital Malformations of The Female Genital TractDo le QuangNoch keine Bewertungen
- PenisDokument23 SeitenPenisWira DharmaNoch keine Bewertungen
- Fertilisasi Askeb IDokument19 SeitenFertilisasi Askeb IPutry Utami0% (1)
- Kipp Mandatory Penis InspectionDokument1 SeiteKipp Mandatory Penis InspectionJeff barkerNoch keine Bewertungen
- Male and Female Infertility GuideDokument35 SeitenMale and Female Infertility GuideJalajarani AridassNoch keine Bewertungen
- Sign of Hyperandrogenism PDFDokument6 SeitenSign of Hyperandrogenism PDFmisbah_mdNoch keine Bewertungen
- StratOG Vaginal BreechDokument17 SeitenStratOG Vaginal BreechNalin AbeysingheNoch keine Bewertungen
- Malereproductive (Author T.globa)Dokument40 SeitenMalereproductive (Author T.globa)Cristina caimac100% (1)
- 3 - Precocious PubertyDokument9 Seiten3 - Precocious PubertyJohnM.GiraldoNoch keine Bewertungen
- I-3 Pediatric and Adolescent GynecologyDokument8 SeitenI-3 Pediatric and Adolescent GynecologyuvioscribdNoch keine Bewertungen
- Female Reproductive SystemDokument6 SeitenFemale Reproductive SystemAlyanna L. ArquillanoNoch keine Bewertungen
- WP GynaeExams4Dokument37 SeitenWP GynaeExams4Ahsan JamNoch keine Bewertungen
- Pre-Operative Conference Anesthetic Considerations For Laryngectomy and Total Thyroidectomy in GeriatricsDokument4 SeitenPre-Operative Conference Anesthetic Considerations For Laryngectomy and Total Thyroidectomy in GeriatricsBhi-An BatobalonosNoch keine Bewertungen
- Morbidity and MortalityDokument2 SeitenMorbidity and MortalityBhi-An BatobalonosNoch keine Bewertungen
- Pedia Census: Ruby Anne D. BatobalonosDokument57 SeitenPedia Census: Ruby Anne D. BatobalonosBhi-An BatobalonosNoch keine Bewertungen
- CP# CP Eval: Covid RT-PCR: CCDokument2 SeitenCP# CP Eval: Covid RT-PCR: CCBhi-An BatobalonosNoch keine Bewertungen
- Preop Conference AnesthesiaDokument33 SeitenPreop Conference AnesthesiaBhi-An BatobalonosNoch keine Bewertungen
- Clinical Clerks Report Case PresDokument8 SeitenClinical Clerks Report Case PresBhi-An BatobalonosNoch keine Bewertungen
- Respiratory Function in Anesthesia: Ruby Anne D. Batobalonos, M.D Anesthesia Pre ResidentDokument17 SeitenRespiratory Function in Anesthesia: Ruby Anne D. Batobalonos, M.D Anesthesia Pre ResidentBhi-An BatobalonosNoch keine Bewertungen
- Protocol LaryngectomyDokument3 SeitenProtocol LaryngectomyBhi-An BatobalonosNoch keine Bewertungen
- Application in ResDokument1 SeiteApplication in ResBhi-An BatobalonosNoch keine Bewertungen
- Organ Dysfunction in SepsisDokument20 SeitenOrgan Dysfunction in SepsisBhi-An BatobalonosNoch keine Bewertungen
- Anesthetic Implications of Guillain-Barre Syndrome in PregnancyDokument34 SeitenAnesthetic Implications of Guillain-Barre Syndrome in PregnancyBhi-An BatobalonosNoch keine Bewertungen
- Pedia Census 5Dokument62 SeitenPedia Census 5Bhi-An BatobalonosNoch keine Bewertungen
- Screenshot 2022-01-24 at 11.15.59 AMDokument1 SeiteScreenshot 2022-01-24 at 11.15.59 AMBhi-An BatobalonosNoch keine Bewertungen
- Pedia Census ArrythmiaDokument48 SeitenPedia Census ArrythmiaBhi-An BatobalonosNoch keine Bewertungen
- NORA Case 2Dokument3 SeitenNORA Case 2Bhi-An BatobalonosNoch keine Bewertungen
- Case Management Conference: Department of Anesthesiology April 19, 2021Dokument8 SeitenCase Management Conference: Department of Anesthesiology April 19, 2021Bhi-An BatobalonosNoch keine Bewertungen
- SynchronousDokument4 SeitenSynchronousBhi-An BatobalonosNoch keine Bewertungen
- Basic ReportDokument1 SeiteBasic ReportBhi-An BatobalonosNoch keine Bewertungen
- Blunt Trauma Abdomen: (Operative V/S Conservative Management)Dokument41 SeitenBlunt Trauma Abdomen: (Operative V/S Conservative Management)Bhi-An BatobalonosNoch keine Bewertungen
- Interesting Case Report Hepatectomy DR B Perez2Dokument10 SeitenInteresting Case Report Hepatectomy DR B Perez2Bhi-An BatobalonosNoch keine Bewertungen
- Anesthetic Management of Non-Fasted Patients Requiring Emergency SurgeryDokument17 SeitenAnesthetic Management of Non-Fasted Patients Requiring Emergency SurgeryBhi-An BatobalonosNoch keine Bewertungen
- Regional Anesthesia - FinalDokument46 SeitenRegional Anesthesia - Finalvan016_bunnyNoch keine Bewertungen
- Guidelines For The Management of AsymptomaticDokument9 SeitenGuidelines For The Management of AsymptomaticBhi-An BatobalonosNoch keine Bewertungen
- Pediatric AnesthDokument213 SeitenPediatric AnesthJyoti Agarwal BhallaNoch keine Bewertungen
- Census - High SpinalDokument30 SeitenCensus - High SpinalBhi-An BatobalonosNoch keine Bewertungen
- Wide Excision With Frozen Section of Malignant Neoplasm Righ Flank July 1Dokument2 SeitenWide Excision With Frozen Section of Malignant Neoplasm Righ Flank July 1Bhi-An BatobalonosNoch keine Bewertungen
- Carbon Cycle Game Worksheet - EportfolioDokument2 SeitenCarbon Cycle Game Worksheet - Eportfolioapi-264746220Noch keine Bewertungen
- TSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideDokument6 SeitenTSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideNavjot KaurNoch keine Bewertungen
- T1D Report September 2023Dokument212 SeitenT1D Report September 2023Andrei BombardieruNoch keine Bewertungen
- Rise School of Accountancy Test 08Dokument5 SeitenRise School of Accountancy Test 08iamneonkingNoch keine Bewertungen
- AnxietyDokument5 SeitenAnxietydrmadankumarbnysNoch keine Bewertungen
- Morningstar Bakery: Business PlanDokument14 SeitenMorningstar Bakery: Business PlanbakhtawarNoch keine Bewertungen
- Bibie Evana OsmanDokument6 SeitenBibie Evana OsmanStabat Jaya TrademarkNoch keine Bewertungen
- Grade 9 P.EDokument16 SeitenGrade 9 P.EBrige SimeonNoch keine Bewertungen
- Vacuum Conveyin 5.0Dokument56 SeitenVacuum Conveyin 5.0Mostafa AtwaNoch keine Bewertungen
- Density of Aggregates: ObjectivesDokument4 SeitenDensity of Aggregates: ObjectivesKit Gerald EliasNoch keine Bewertungen
- Darnell's Father Goes StrictDokument2 SeitenDarnell's Father Goes StrictDavid Theodore Richardson IIINoch keine Bewertungen
- Platinum Gazette 29 November 2013Dokument12 SeitenPlatinum Gazette 29 November 2013Anonymous w8NEyXNoch keine Bewertungen
- ZP Series Silicon Rectifier: Standard Recovery DiodesDokument1 SeiteZP Series Silicon Rectifier: Standard Recovery DiodesJocemar ParizziNoch keine Bewertungen
- Gsis - Ra 8291Dokument33 SeitenGsis - Ra 8291RoySantosMoralesNoch keine Bewertungen
- Informática Ejercicios IDokument10 SeitenInformática Ejercicios IAlejandroMendezNoch keine Bewertungen
- Edna Adan University ThesisDokument29 SeitenEdna Adan University ThesisAbdi KhadarNoch keine Bewertungen
- The Bresle Method: Improving Accuracy of Soluble Salt MeasurementsDokument4 SeitenThe Bresle Method: Improving Accuracy of Soluble Salt MeasurementsMuthuKumarNoch keine Bewertungen
- Berman Et Al-2019-Nature Human BehaviourDokument5 SeitenBerman Et Al-2019-Nature Human BehaviourMira mNoch keine Bewertungen
- 3.SAFA AOCS 4th Ed Ce 2-66 1994Dokument6 Seiten3.SAFA AOCS 4th Ed Ce 2-66 1994Rofiyanti WibowoNoch keine Bewertungen
- 1 The Fifth CommandmentDokument10 Seiten1 The Fifth CommandmentSoleil MiroNoch keine Bewertungen
- Kidde Ads Fm200 Design Maintenance Manual Sept 2004Dokument142 SeitenKidde Ads Fm200 Design Maintenance Manual Sept 2004José AravenaNoch keine Bewertungen
- Notes Lecture No 3 Cell Injury and MechanismDokument5 SeitenNotes Lecture No 3 Cell Injury and MechanismDr-Rukhshanda RamzanNoch keine Bewertungen