Das könnte Ihnen auch gefallen
- Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformVon EverandMeeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformAmy S. KelleyNoch keine Bewertungen
- Access To Health Care Services For The Disabled Elderly: Donald H. Taylor, Jr. and Helen HoenigDokument17 SeitenAccess To Health Care Services For The Disabled Elderly: Donald H. Taylor, Jr. and Helen HoenighkuruputNoch keine Bewertungen
- HCM2005 Healthcare Delivery and Organization2Dokument3 SeitenHCM2005 Healthcare Delivery and Organization2fredrickm kamau2017Noch keine Bewertungen
- Fenton (2012) - The Cost of Satisfaction - A National Study of Patient Satisfaction, Health Care Utilization, Expenditures, and MortalityDokument7 SeitenFenton (2012) - The Cost of Satisfaction - A National Study of Patient Satisfaction, Health Care Utilization, Expenditures, and Mortalityghcabsb87Noch keine Bewertungen
- The Importance of Health Literacy in Physiotherapy Practice: Andrew M Briggs and Joanne E JordanDokument3 SeitenThe Importance of Health Literacy in Physiotherapy Practice: Andrew M Briggs and Joanne E JordanMhmd IrakyNoch keine Bewertungen
- Limited Access To Health CareDokument5 SeitenLimited Access To Health CarezeeshanNoch keine Bewertungen
- Policy Brief CompleteDokument3 SeitenPolicy Brief Completeapi-301033624Noch keine Bewertungen
- Medicare The How and WhyDokument10 SeitenMedicare The How and WhyKaren JonesNoch keine Bewertungen
- Medicine and Health - EditedDokument5 SeitenMedicine and Health - EditedAlex WafulaNoch keine Bewertungen
- Nurse Practitioner Independence, Health Care Utilization, and Health OutcomesDokument46 SeitenNurse Practitioner Independence, Health Care Utilization, and Health OutcomesDavid WheelerNoch keine Bewertungen
- Disaster 3 Ijerph 15 01879 v2Dokument29 SeitenDisaster 3 Ijerph 15 01879 v2Devi SiswaniNoch keine Bewertungen
- Chapter II Review of Related LiteratureDokument15 SeitenChapter II Review of Related Literaturemtalquisola2002Noch keine Bewertungen
- Improving Acheiving Health EquityDokument16 SeitenImproving Acheiving Health EquityCale HollowayNoch keine Bewertungen
- 1ausing Information Systems To Improve Population Outcomes Concepts in Program Design and Development Structure SystemsDokument7 Seiten1ausing Information Systems To Improve Population Outcomes Concepts in Program Design and Development Structure Systemsapi-678571963Noch keine Bewertungen
- Policy Action PlanDokument10 SeitenPolicy Action Planapi-541665858Noch keine Bewertungen
- Unit 7 Computer ApplicationsDokument5 SeitenUnit 7 Computer ApplicationsBea Bianca CruzNoch keine Bewertungen
- AbstractDokument36 SeitenAbstractJackson MwaiNoch keine Bewertungen
- Health Disparities and Health Education-1finalDokument12 SeitenHealth Disparities and Health Education-1finalbrendahronoh254Noch keine Bewertungen
- Wtrp5-Influences On Care DeliveryDokument24 SeitenWtrp5-Influences On Care DeliveryKATHYANN HOLDERNoch keine Bewertungen
- Notes and Editing Sheet2Dokument3 SeitenNotes and Editing Sheet2Christian HawthorneNoch keine Bewertungen
- Zhen Duan2021Dokument10 SeitenZhen Duan2021Epigmenio Díaz CruzNoch keine Bewertungen
- Barriers To Access Quality Healthcare Services Among Physically Challenged Persons in Gem Sub County, Siaya County'Dokument9 SeitenBarriers To Access Quality Healthcare Services Among Physically Challenged Persons in Gem Sub County, Siaya County'Premier PublishersNoch keine Bewertungen
- Research ProposalDokument7 SeitenResearch ProposalTony DumfehNoch keine Bewertungen
- Tito IRBRPDokument13 SeitenTito IRBRPTito TiehiNoch keine Bewertungen
- Module SummaryDokument3 SeitenModule SummaryKen EdwardsNoch keine Bewertungen
- Too Frightened To Care Accounts by District Nurses Working With Clients Who Misuse SubstancesDokument8 SeitenToo Frightened To Care Accounts by District Nurses Working With Clients Who Misuse SubstancesNadeen WilliamsNoch keine Bewertungen
- HLTH 101 PaperDokument8 SeitenHLTH 101 Paperapi-548493910Noch keine Bewertungen
- How Effective Is Capitation at Reducing Health Care CostsDokument6 SeitenHow Effective Is Capitation at Reducing Health Care CostsIndah ShofiyahNoch keine Bewertungen
- Hospice and Self-Assessed Quality of Life in The Dying: A ReviewDokument16 SeitenHospice and Self-Assessed Quality of Life in The Dying: A Reviewrohmana kusnul adzaniNoch keine Bewertungen
- 2015 Article 161 PDFDokument7 Seiten2015 Article 161 PDFPearl EmmarossNoch keine Bewertungen
- Running Head: Analyzes The Need For Health Care Reform 1Dokument5 SeitenRunning Head: Analyzes The Need For Health Care Reform 1Pennie DavisNoch keine Bewertungen
- HCM 340 7-2Dokument11 SeitenHCM 340 7-2Robin McFaddenNoch keine Bewertungen
- The Relationship Between Insurance and Health Outcomes of Diabetes Mellitus Patients in Maryland: A Retrospective Archival Record StudyDokument10 SeitenThe Relationship Between Insurance and Health Outcomes of Diabetes Mellitus Patients in Maryland: A Retrospective Archival Record StudyFINDRI FADLIKANoch keine Bewertungen
- Social Factors Influencing Individual and Population Health - EditedDokument6 SeitenSocial Factors Influencing Individual and Population Health - EditedOkoth OluochNoch keine Bewertungen
- Healthcare Policy Names InstitutionDokument29 SeitenHealthcare Policy Names InstitutionMaestro WritersNoch keine Bewertungen
- Estimating The Underestimation Profile of Health Service Need S Through Telephone Counseling CentersDokument13 SeitenEstimating The Underestimation Profile of Health Service Need S Through Telephone Counseling Centersנבט כהןNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument16 SeitenNIH Public Access: Author Manuscriptashgee1Noch keine Bewertungen
- Paper 1Dokument10 SeitenPaper 1lsnzgiNoch keine Bewertungen
- Ethical Case Analysis PaperDokument14 SeitenEthical Case Analysis Paperapi-282129457100% (1)
- HSM541 FinalDokument5 SeitenHSM541 Finalteekel_1125Noch keine Bewertungen
- 1 PDFDokument19 Seiten1 PDFDoni DarcoNoch keine Bewertungen
- RehabilitationDokument10 SeitenRehabilitationasuratosNoch keine Bewertungen
- National Health Insurance FailureDokument4 SeitenNational Health Insurance FailureGaddafi PhelixNoch keine Bewertungen
- Interfaces Between The Aged Care and Health Systems in Australia-First ResultsDokument16 SeitenInterfaces Between The Aged Care and Health Systems in Australia-First ResultsNgân Hàng Ngô Mạnh TiếnNoch keine Bewertungen
- Week 10 Patient Centered CareDokument30 SeitenWeek 10 Patient Centered CareNermine ElcokanyNoch keine Bewertungen
- 15 Finkelstein Et Al 2012 Oregon Insurance ExperimentDokument50 Seiten15 Finkelstein Et Al 2012 Oregon Insurance ExperimentprithvijitmNoch keine Bewertungen
- Occupational Therapy Service Delivery Among Medicaid-Enrolled Children and Adults On The Autism Spectrum and With Other Intellectual DisabilitiesDokument9 SeitenOccupational Therapy Service Delivery Among Medicaid-Enrolled Children and Adults On The Autism Spectrum and With Other Intellectual DisabilitiesNataliaNoch keine Bewertungen
- Care Services By: Factors Explaining The Use of Health The ElderlyDokument26 SeitenCare Services By: Factors Explaining The Use of Health The ElderlyYonis Dhey BebheNoch keine Bewertungen
- Allied Health Scenario (AHS)Dokument4 SeitenAllied Health Scenario (AHS)Johnson JayNoch keine Bewertungen
- No 362524 3Dokument5 SeitenNo 362524 3My EscrowNoch keine Bewertungen
- Caribbean Studies IA 1Dokument11 SeitenCaribbean Studies IA 1mario josephNoch keine Bewertungen
- US Healthcare SystemDokument6 SeitenUS Healthcare SystemEmmi JeanNoch keine Bewertungen
- SSM - Qualitative Research in HealthDokument10 SeitenSSM - Qualitative Research in HealthDWI HERU CAHYONONoch keine Bewertungen
- Health Access and Quality DeterminantsDokument17 SeitenHealth Access and Quality DeterminantsCharley WatebaNoch keine Bewertungen
- Demand in Health Care AnalysisDokument9 SeitenDemand in Health Care AnalysisZewdu MinwuyeletNoch keine Bewertungen
- BAREMDokument9 SeitenBAREMbaremayubaNoch keine Bewertungen
- Private Versus Public Provision of Social Insurance: Evidence From MedicaidDokument3 SeitenPrivate Versus Public Provision of Social Insurance: Evidence From MedicaidCato InstituteNoch keine Bewertungen
- Andersen Theory of HC UtilizationDokument28 SeitenAndersen Theory of HC UtilizationKukuh ArdianNoch keine Bewertungen
- Community Health Concepts NotesDokument7 SeitenCommunity Health Concepts Noteswano chioneNoch keine Bewertungen
- Hall Flows Hospitals Chapter1text PDFDokument45 SeitenHall Flows Hospitals Chapter1text PDFShin BoyceNoch keine Bewertungen
- Effects of Alcohol, Tobacco, and Marijuana - PR 1Dokument11 SeitenEffects of Alcohol, Tobacco, and Marijuana - PR 1Mark Andris GempisawNoch keine Bewertungen
- The Role of Financial System in DevelopmentDokument5 SeitenThe Role of Financial System in DevelopmentCritical ThinkerNoch keine Bewertungen
- Software Project Management PDFDokument125 SeitenSoftware Project Management PDFUmirNoch keine Bewertungen
- Resume of Masterchef Contestant, Melissa GutierrezDokument3 SeitenResume of Masterchef Contestant, Melissa GutierrezMikhail GalatinovNoch keine Bewertungen
- Chemiphase Oilfield Demulsifier Testing ProcedureDokument4 SeitenChemiphase Oilfield Demulsifier Testing ProcedureBen Wiggins100% (1)
- Midterm Decision Analysis ExercisesDokument5 SeitenMidterm Decision Analysis ExercisesAYLEN INJAYANoch keine Bewertungen
- Analysing Worship in The Pentateuch and Its ApplicationDokument12 SeitenAnalysing Worship in The Pentateuch and Its ApplicationDaniel Solomon100% (1)
- Bubble ColumnDokument34 SeitenBubble ColumnihsanNoch keine Bewertungen
- Habanera Botolena & Carinosa (Gas-A)Dokument8 SeitenHabanera Botolena & Carinosa (Gas-A)christian100% (4)
- Character Formation 1: Nationalism and PatriotismDokument11 SeitenCharacter Formation 1: Nationalism and Patriotismban diaz100% (1)
- Bug Tracking System AbstractDokument3 SeitenBug Tracking System AbstractTelika Ramu86% (7)
- Contracts ChecklistDokument3 SeitenContracts ChecklistSteve WatmoreNoch keine Bewertungen
- Bsed FilipinoDokument18 SeitenBsed FilipinoJ.PNoch keine Bewertungen
- Sample Internship PPTDokument19 SeitenSample Internship PPTSangeeta JamadarNoch keine Bewertungen
- IUGRDokument4 SeitenIUGRMichael Spica RampangileiNoch keine Bewertungen
- Thesis Committee MeetingDokument7 SeitenThesis Committee Meetingafknojbcf100% (2)
- Class 12 Accountancy HHDokument58 SeitenClass 12 Accountancy HHkomal barotNoch keine Bewertungen
- Linking and Relocation - Stacks - Procedures - MacrosDokument11 SeitenLinking and Relocation - Stacks - Procedures - MacrosJeevanantham GovindarajNoch keine Bewertungen
- Names of AllahDokument8 SeitenNames of AllahAfshaan BanuNoch keine Bewertungen
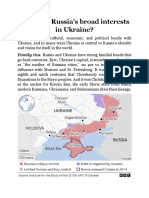
- What Are RussiaDokument3 SeitenWhat Are RussiaMuhammad SufyanNoch keine Bewertungen
- Scipaper 7Dokument2 SeitenScipaper 7JL Serioso BalesNoch keine Bewertungen
- Fallopian Tube BlockageDokument11 SeitenFallopian Tube Blockagesimran kaurNoch keine Bewertungen
- Electronic Load FundamentalsDokument16 SeitenElectronic Load FundamentalsMiguel PenarandaNoch keine Bewertungen
- WHO CDS HIV 19.8 EngDokument24 SeitenWHO CDS HIV 19.8 EngMaykel MontesNoch keine Bewertungen
- Analysis of Low-Frequency Passive Seismic Attributes in Maroun Oil Field, IranDokument16 SeitenAnalysis of Low-Frequency Passive Seismic Attributes in Maroun Oil Field, IranFakhrur NoviantoNoch keine Bewertungen
- Ccounting Basics and Interview Questions AnswersDokument18 SeitenCcounting Basics and Interview Questions AnswersAamir100% (1)
- Polynomials Level 3Dokument17 SeitenPolynomials Level 3greycouncilNoch keine Bewertungen
- GST 101 Exam Past QuestionsDokument6 SeitenGST 101 Exam Past QuestionsBenjamin Favour100% (2)
- Match The Animal With Its NameDokument4 SeitenMatch The Animal With Its Namekawa kawka kawuniaNoch keine Bewertungen
- Asset Management PlanDokument160 SeitenAsset Management Planbkalatus1100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (28)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- 1177 B.C.: The Year Civilization Collapsed: Revised and UpdatedVon Everand1177 B.C.: The Year Civilization Collapsed: Revised and UpdatedBewertung: 4.5 von 5 Sternen4.5/5 (111)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndVon EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndNoch keine Bewertungen
- Selling the Dream: The Billion-Dollar Industry Bankrupting AmericansVon EverandSelling the Dream: The Billion-Dollar Industry Bankrupting AmericansBewertung: 4 von 5 Sternen4/5 (17)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldVon EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldBewertung: 4.5 von 5 Sternen4.5/5 (1145)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- The Wicked and the Willing: An F/F Gothic Horror Vampire NovelVon EverandThe Wicked and the Willing: An F/F Gothic Horror Vampire NovelBewertung: 4 von 5 Sternen4/5 (21)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Hey, Hun: Sales, Sisterhood, Supremacy, and the Other Lies Behind Multilevel MarketingVon EverandHey, Hun: Sales, Sisterhood, Supremacy, and the Other Lies Behind Multilevel MarketingBewertung: 4 von 5 Sternen4/5 (103)
- The Other Significant Others: Reimagining Life with Friendship at the CenterVon EverandThe Other Significant Others: Reimagining Life with Friendship at the CenterBewertung: 4 von 5 Sternen4/5 (1)
- Troubled: The Failed Promise of America’s Behavioral Treatment ProgramsVon EverandTroubled: The Failed Promise of America’s Behavioral Treatment ProgramsBewertung: 5 von 5 Sternen5/5 (2)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Troubled: A Memoir of Foster Care, Family, and Social ClassVon EverandTroubled: A Memoir of Foster Care, Family, and Social ClassBewertung: 4.5 von 5 Sternen4.5/5 (27)
- The Exvangelicals: Loving, Living, and Leaving the White Evangelical ChurchVon EverandThe Exvangelicals: Loving, Living, and Leaving the White Evangelical ChurchBewertung: 4.5 von 5 Sternen4.5/5 (13)
- American Jezebel: The Uncommon Life of Anne Hutchinson, the Woman Who Defied the PuritansVon EverandAmerican Jezebel: The Uncommon Life of Anne Hutchinson, the Woman Who Defied the PuritansBewertung: 3.5 von 5 Sternen3.5/5 (66)
- If I Did It: Confessions of the KillerVon EverandIf I Did It: Confessions of the KillerBewertung: 3 von 5 Sternen3/5 (133)
- Little Princes: One Man's Promise to Bring Home the Lost Children of NepalVon EverandLittle Princes: One Man's Promise to Bring Home the Lost Children of NepalNoch keine Bewertungen
- Body Language: Decode Human Behaviour and How to Analyze People with Persuasion Skills, NLP, Active Listening, Manipulation, and Mind Control Techniques to Read People Like a Book.Von EverandBody Language: Decode Human Behaviour and How to Analyze People with Persuasion Skills, NLP, Active Listening, Manipulation, and Mind Control Techniques to Read People Like a Book.Bewertung: 5 von 5 Sternen5/5 (81)
- The Pursuit of Happyness: The Life Story That Inspired the Major Motion PictureVon EverandThe Pursuit of Happyness: The Life Story That Inspired the Major Motion PictureNoch keine Bewertungen
- The Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionVon EverandThe Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionBewertung: 4 von 5 Sternen4/5 (812)