
Poster Abstracts
Thursday 14 August 2008
CONCURRENT ORAL SESSION 155: LATE BREAKING
POSTER BOARD NUMBER P4 373
2323 POST TRANSPLANTATION LYMPHOPROLIFERATIVE
DISORDER AFTER LIVER TRANSPLANTATION: A SINGLE
CENTER EXPERIENCE AMONG 400 PATIENT SERIES
S. Marzban, B. Geramizadeh, S-A. Malek-Hosseini, A. Bahador, H. Salahi, K.
Bagheri-Lankarani, M-H. Imanieh
Transplant Research Center, Shiraz University of Medical Sciences
Introduction: Post transplant lymphoproliferative disorders (PTLD) are a
heterogenous group of lymphoid proliferation occurring in the setting of solid
organ or BM transplantation.
In this review we will consider the incidence and clinical features of this group
of patients in our center.
Material and Methods: In this study, we present the clinical and pathologic
features of PTLD cases after liver transplantation (LT). In the period of liver
transplantation we had 3 pathology conrmed cases of PTLD out of 430 liver
transplant cases.
Results: Among 430 liver transplantation 3 cases were diagnosed as PTLD. Two
of the patients were child (both 6 year-old) and the other was adult (45 year-old).
One of the children was presented with diarrhea after 6 months of transplant and
PTLD (polymorphic type) was diagnosed on duodenal biopsy, she expired despite
of reducing the immunosuppressive therapy and starting of chemotherapy. The
other child was present with cervical lymphadenopathy one year after transplant.
He was also expired. The reason of liver transplantation was biliary atresia in
both of them. The last one was an HCV positive male patient who presented
with a very small cervical lymphnode( 1 cm) 1 year after liver transplant. He was
diagnosed as Hodgkins-like type of PTLD, now after 3 years he is doing well. In
all the three case EBV was positive in the involved tissue.
Conclusion: In conclusion, PTLD is a life treating disorder in liver transplant
patients. According to the present data (3/430) it seems that the incidence of
this disorder is lower than other parts of the world.
POSTER BOARD NUMBER P4 374
2324 ASSESSMENT OF CAUSATIVE FACTORS FOR
LYMPHOCELE FORMATION FOLLOWING RENAL
TRANSPLANTATION
J. Kothari, H. Talreja, A. Supariwala, R. Sirsat, A. Almeida
Pd Hinduja Hospital
Introduction: Lymphocele is a uid collection between the renal graft and the
urinary bladder. It is an uncommon complication (0.6% to 18%) following renal
transplantation. It is associated with incomplete ligation of lymphatic vessels
of graft, extensive perivascular dissection in the recipient, acute rejection and
use of high dose steroids.
Objective: To determine the incidence of lymphocele in post renal transplant
patients at our center and identify potential factors responsible or associated to
its development.
Materials and Methods: All patients who underwent renal transplantation at
our centre from Jan 2004 to Oct 2007 with complete medical records were
reviewed.
Results: Out of 138 patients who had undergone renal transplantation, 48
developed lymphocele(34.7%).28 patients (58%) required surgical drainage
or pigtail catherization. Signicant variation was noted in yearly incidence of
lymphocele which coincided with the yearly change in the surgical registrar
preparing the bed for the recipient. Signicantly, 25 out of 52 patients with
urinary tract infection developed lymphocele as compared to 23 out of 86
without evidence of urinary infection (p=0.016) . A total of 25 Acute rejection
episodes was seen in total with similar incidence in the two groups, with &
without lymphocele. Gram negative bacteria causing UTI, especially those
resistant to beta lactam antibiotics (ESBL) were the commonest organisms
isolated in patients with lymphocele formation.Use of IL-2R antagonists for
induction was not associated with increased incidence of lymphocele. There is
no association of lymphocele formation with the different immunosuppressive
regimens used at our center. Diabetic patients had a higher incidence of
lymphocele, but the difference was statistically insignicant (p=0.056).
Conclusion: More attention to careful ligation of lymphatic vessels both during
graft bed preparation and during graft implantation can signicantly contribute
to reducing the incidence of lymphocele following renal transplantation. Cases
requiring surgical treatment cause signicant morbidity. Preventive methods,
such as laparoscopic fenestration need to be done routinely to minimise
lymphocele formation. Urinary infections post-transplant is associated with
increased incidence of lymphocele formation. Diabetics may be more prone
for higher lymph collection, probably due to delayed healing of the dissected
lymphatics, but that remains to be proven conclusively.
POSTER BOARD NUMBER P4 375
2325 LAPAROTOMIC LIVE DONOR NEPHRECTOMY: IS IT
STILL JUSTIFIED?
M.A. Zargar, H. Shahrokh, M.J. Soleimani, K. Kamali, S.K. Hosseini, S.M.R.
Rabani, A. Barzegarnejad, E. Azimi
Shaheed Hasheminejad Hospital, Iran University of Medical Sciences
Purpose: We report our experience with laparatomic Live Donor Nephretomy
during the last 23 years.
Patents and methods: Between August 1985 and November 2007, 2260
consecutive live donors who underwent laparatomic nephrectomy at the
university hospital of Hasheminejad in Tehran, were included in this audit.
All donors underwent routine preoperative assessments including renal
angiography, to evaluate the anatomy of the renal arteries. Patients underwent
a high midline laparatomy under general anesthesia. Principally the left kidney
was the preferred side unless multiple left sided renal arteries were present.
For the left kidney, in most cases, the inferior mesenteric vein was ligated and
the retroperitoneum entered with a good access to left kidney and its pedicle.
On the right side after duodenal kocherization, the right kidney and its pedicel
were easily accessible. After removal of the kidney the posterior peritoneum
defect is closed and a short term drain is placed.
Result: 2260 live donors underwent laparatomy during a period of near 23
years. They were 1440 male and 820 female. Left kidney was used in 95% of
the cases. The mean donor age was 26 years (20-48 years). The mean hospital
stay was 3 days (2-5 days). The mean incisional length was 12 cm ( 2.5 cm).
The mean warm ischemia time was always less than 1 minute. The mean
operation time was 55 minutes (40-70 minutes). The mean intraoperative blood
loss was 200mls and there were no post operative transfusions. There were no
signicant gastrointestinal complications. Postoperative morality occurred in
one case with sudden death of a 31 years old male who developed abdominal
pain 16 hours after operation. He was suspected of massive bleeding from renal
artery stump. Incision hernia in four cases, which required operative repair.
Signicant lymphocele occurred in one case, which responded well to surgical
intervention.
Conclusion: In our experience midline laparatomy, is a very safe and efcacious
approach for live donor nephrectomy. It is associated with short operative
time and low morbidity rates and despite the rapid development of minimally
invasive techniques, this approach will continue to have a denite place in high
volume units such as ours. In our experience the only long-term disadvantage
of laparatomic donor nephrectomy has been in the cosmetic results.
POSTER BOARD NUMBER P4 376
2326 PROTEIN TRANSDUCTION TECHNOLOGY FOR STEM
CELL REPROGRAMMING: A NOVEL STRATEGY TO OBTAIN
INSULIN-PRODUCING CELLS
M. Ramrez-Domnguez1,2, N. Vicente-Salar2, A. Santana3, J. DomnguezBendala1, L. Inverardi1, C. Ricordi1, K. Hmadcha4, B. Soria4, E. Roche2
1
Diabetes Research Institute. University of Miami, 2 Instituto de
Bioingenieria.Universidad Miguel Hernandez de Elche, Spain, 3 Hospital
Universitario de Las Palmas, Spain, 4 Centro Andaluz de Biologia Molecular
y Medicina Regenerativa (CABIMER), Sevilla, Spain
Several reports have demonstrated the potential of mouse and human embryonic
stem (ES) cells to differentiate into insulin-producing cells and revert diabetes
in transplanted animal models. However, in vitro protocols are still inefcient,
as they give rise to heterogeneous cell populations that include undifferentiated
cells and derivatives of the three embryonic layers. Thus, there is a need for
alternative approaches to improve the efciency of beta cell differentiation.
The feasibility of reprogramming strategies has already been demonstrated.
759
THURSDAY
Supplement to Transplantation July 27, 2008, Volume 86 Number 2S
Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- tmpF178 TMPDokument15 SeitentmpF178 TMPFrontiersNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Tmp1a96 TMPDokument80 SeitenTmp1a96 TMPFrontiersNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- tmpE3C0 TMPDokument17 SeitentmpE3C0 TMPFrontiersNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Tmpa077 TMPDokument15 SeitenTmpa077 TMPFrontiersNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- tmp998 TMPDokument9 Seitentmp998 TMPFrontiersNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- tmp27C1 TMPDokument5 Seitentmp27C1 TMPFrontiersNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- tmp3656 TMPDokument14 Seitentmp3656 TMPFrontiersNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- tmpA7D0 TMPDokument9 SeitentmpA7D0 TMPFrontiersNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- tmp96F2 TMPDokument4 Seitentmp96F2 TMPFrontiersNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- tmp97C8 TMPDokument9 Seitentmp97C8 TMPFrontiersNoch keine Bewertungen
- Chest Pain Algorithm Clinical Case Scenarios PDF 243970669Dokument28 SeitenChest Pain Algorithm Clinical Case Scenarios PDF 243970669Romelu MartialNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Constrictive PericarditisDokument5 SeitenConstrictive Pericarditisvicky3101Noch keine Bewertungen
- Table of Contents - YjomsDokument6 SeitenTable of Contents - YjomsSUMEET SODHINoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
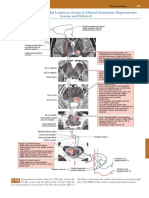
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDokument1 SeitePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- 2-NPSG Chapter OBS Jan2023Dokument8 Seiten2-NPSG Chapter OBS Jan2023Blanca LanderosNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Poster PresentationsDokument3 SeitenPoster PresentationsdocbinNoch keine Bewertungen
- Neuro DisordersDokument159 SeitenNeuro DisordersQuolette Constante100% (1)
- Soal-Soal Teori Trauma ExamDokument4 SeitenSoal-Soal Teori Trauma ExamAkai KiriNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Starting An Intravenous InfusionDokument2 SeitenStarting An Intravenous InfusionAmiel Francisco Reyes100% (1)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- When To Implant ICD in Post MI PatientDokument36 SeitenWhen To Implant ICD in Post MI PatientCarissa CkNoch keine Bewertungen
- Dialysis Application For LTO Rev1 1232014Form-HDC-LTO-A-2007Dokument12 SeitenDialysis Application For LTO Rev1 1232014Form-HDC-LTO-A-2007al gulNoch keine Bewertungen
- Management of Breast Cancer: Yonas Ademe April, 2019Dokument66 SeitenManagement of Breast Cancer: Yonas Ademe April, 2019moges beletachawNoch keine Bewertungen
- Choque HemorragicoDokument9 SeitenChoque HemorragicoAna NevesNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Budget Plan Wound ClinicDokument4 SeitenBudget Plan Wound ClinicRegalado Aguhayon100% (1)
- Laparaskopi HTDokument167 SeitenLaparaskopi HTbarsitom100% (1)
- Ulcerative ColitisDokument18 SeitenUlcerative ColitisKyle Ü D. CunanersNoch keine Bewertungen
- Reviewer - CamcaDokument11 SeitenReviewer - CamcaLouise Andrea OdulioNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Phaco Machine Procedure PDFDokument4 SeitenPhaco Machine Procedure PDFAlim SumonNoch keine Bewertungen
- Nuclear Medicin IdafDokument19 SeitenNuclear Medicin IdafSaifNoch keine Bewertungen
- R Series Operator's Guide: 9650-0912-01 Rev. VDokument178 SeitenR Series Operator's Guide: 9650-0912-01 Rev. VA. A.G.Noch keine Bewertungen
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDokument12 SeitenThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNoch keine Bewertungen
- Guideline_for_the_Management_of_HyaluronDokument9 SeitenGuideline_for_the_Management_of_HyaluronTHIEN NGUYENNoch keine Bewertungen
- Expert DDX ChestDokument1.053 SeitenExpert DDX ChestClaudio Rodriguez100% (1)
- Description:: Materials/ Equipment NeededDokument6 SeitenDescription:: Materials/ Equipment NeededMarc Renz R. ChanNoch keine Bewertungen
- Medical Apparatus That Can Help Control DiseasesDokument3 SeitenMedical Apparatus That Can Help Control DiseasesKrista-Ann KhoNoch keine Bewertungen
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KDokument60 SeitenChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasNoch keine Bewertungen
- UNIT 1 - The Human BodyDokument27 SeitenUNIT 1 - The Human BodyEricBuguinaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mks 054Dokument7 SeitenMks 054Mirela CiobanescuNoch keine Bewertungen
- Chapter 7Dokument7 SeitenChapter 7Mia Kristhyn Calinawagan SabanalNoch keine Bewertungen
- Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, And Endodontology Volume 93 Issue 1 2002 [Doi 10.1067_moe.2002.119519] Norbert Jakse; Vedat Bankaoglu; Gernot Wimmer; Antranik Eskici; -- Primary WounDokument6 SeitenOral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, And Endodontology Volume 93 Issue 1 2002 [Doi 10.1067_moe.2002.119519] Norbert Jakse; Vedat Bankaoglu; Gernot Wimmer; Antranik Eskici; -- Primary WounMr-Ton DrgNoch keine Bewertungen














































































![Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, And Endodontology Volume 93 Issue 1 2002 [Doi 10.1067_moe.2002.119519] Norbert Jakse; Vedat Bankaoglu; Gernot Wimmer; Antranik Eskici; -- Primary Woun](https://imgv2-1-f.scribdassets.com/img/document/224676744/149x198/8c2fa96a30/1400316861?v=1)
