Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Rethinking The Infamous Milgram Experiment in Authoritarian TimesDokument3 SeitenRethinking The Infamous Milgram Experiment in Authoritarian TimesBruna RodriguesNoch keine Bewertungen
- 1.validation of Processes For Production Service Provision ProcedureDokument4 Seiten1.validation of Processes For Production Service Provision ProcedureLora Jackson100% (1)
- Adrenal CrisisDokument6 SeitenAdrenal CrisisSteven SetioNoch keine Bewertungen
- Mural Painting SyllabusDokument4 SeitenMural Painting Syllabusapi-2608097640% (1)
- Leanne E. Atwater, David A. Waldman - Leadership, Feedback and The Open Communication Gap (2007) PDFDokument178 SeitenLeanne E. Atwater, David A. Waldman - Leadership, Feedback and The Open Communication Gap (2007) PDFjanti100% (1)
- Lesson Plan in The K To 12 Basic Education Curriculum and It's Implication To Pre-Service Teacher EducationDokument5 SeitenLesson Plan in The K To 12 Basic Education Curriculum and It's Implication To Pre-Service Teacher EducationJelly Marie Baya Flores67% (3)
- BehaviourismDokument30 SeitenBehaviourismAsma Riaz0% (1)
- RCOG Cardiac Disease and Pregnancy PDFDokument18 SeitenRCOG Cardiac Disease and Pregnancy PDFSteven SetioNoch keine Bewertungen
- Supplementary Table 1a. All Study Data For Bladder Cancer IncidenceDokument19 SeitenSupplementary Table 1a. All Study Data For Bladder Cancer IncidenceSteven SetioNoch keine Bewertungen
- Perforated Jejunal Diverticular Disease: A Diagnostic Pitfall at Frozen Section of A Mesenteric Mass For Adenocarcinoma of The StomachDokument3 SeitenPerforated Jejunal Diverticular Disease: A Diagnostic Pitfall at Frozen Section of A Mesenteric Mass For Adenocarcinoma of The StomachSteven SetioNoch keine Bewertungen
- The Association Between Smoking Quantity and Lung Cancer in Men and WomenDokument7 SeitenThe Association Between Smoking Quantity and Lung Cancer in Men and WomenSteven SetioNoch keine Bewertungen
- RCOG Cardiac Disease and Pregnancy PDFDokument18 SeitenRCOG Cardiac Disease and Pregnancy PDFSteven SetioNoch keine Bewertungen
- Guidlines Pregnancy and Heart DiseaseDokument52 SeitenGuidlines Pregnancy and Heart DiseasePanggih Sekar Palupi IINoch keine Bewertungen
- Status Asmatikus 1Dokument8 SeitenStatus Asmatikus 1Steven SetioNoch keine Bewertungen
- GINA 2016 Main Pocket GuideDokument29 SeitenGINA 2016 Main Pocket GuideKaren Ceballos LopezNoch keine Bewertungen
- ESC Guidelines For DX and TX of Acute and Chronic HF (2016)Dokument85 SeitenESC Guidelines For DX and TX of Acute and Chronic HF (2016)Imja94Noch keine Bewertungen
- Sle 07 PDFDokument6 SeitenSle 07 PDFSteven SetioNoch keine Bewertungen
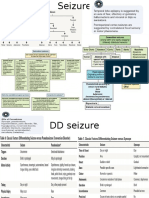
- SeizureDokument6 SeitenSeizureSteven SetioNoch keine Bewertungen
- 1 s2.0 S0735675713004890Dokument3 Seiten1 s2.0 S0735675713004890Steven SetioNoch keine Bewertungen
- Nefrolitiasis 02Dokument8 SeitenNefrolitiasis 02Steven SetioNoch keine Bewertungen
- DR - Jane Gillett-Whats The Difference Between A Subdural and Epidural HematomaDokument2 SeitenDR - Jane Gillett-Whats The Difference Between A Subdural and Epidural HematomaproluvieslacusNoch keine Bewertungen
- International Journal of Gynecology and ObstetricsDokument4 SeitenInternational Journal of Gynecology and ObstetricsSteven SetioNoch keine Bewertungen
- Nefrolitiasis RadiologiDokument9 SeitenNefrolitiasis RadiologiSteven SetioNoch keine Bewertungen
- Sle 05 PDFDokument6 SeitenSle 05 PDFSteven SetioNoch keine Bewertungen
- Frequency Table UnivariatDokument2 SeitenFrequency Table UnivariatSteven SetioNoch keine Bewertungen
- 3 s2.0 B9781437722062001391Dokument23 Seiten3 s2.0 B9781437722062001391Steven SetioNoch keine Bewertungen
- Tugas KKDDokument4 SeitenTugas KKDSteven SetioNoch keine Bewertungen
- Fleis PDFDokument1 SeiteFleis PDFSteven SetioNoch keine Bewertungen
- Performance Task In: Business MathematicsDokument3 SeitenPerformance Task In: Business MathematicsEvone Mariz Tan AzagraNoch keine Bewertungen
- Annex 3 - Gap Analysis Template With Division Targets Based On DEDPDokument15 SeitenAnnex 3 - Gap Analysis Template With Division Targets Based On DEDPJanine Gorday Tumampil BorniasNoch keine Bewertungen
- Daniel Philip: ObjectivesDokument2 SeitenDaniel Philip: ObjectivesAnonymous n3QUDhPv5Noch keine Bewertungen
- UBCSauder RHL OnlineBrochure2023Dokument24 SeitenUBCSauder RHL OnlineBrochure2023Prthm ShrmaNoch keine Bewertungen
- Syllabus in Assessment 1Dokument6 SeitenSyllabus in Assessment 1Julius BalbinNoch keine Bewertungen
- Parent Guide English For Web RevisedDokument32 SeitenParent Guide English For Web RevisedBronxTeacherNoch keine Bewertungen
- Activity Completion Report of Project HopeDokument7 SeitenActivity Completion Report of Project HopeRogelio LadieroNoch keine Bewertungen
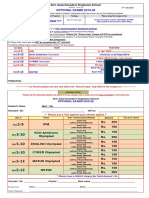
- Optional Exams 2019-20: Smt. Sulochanadevi Singhania SchoolDokument1 SeiteOptional Exams 2019-20: Smt. Sulochanadevi Singhania SchoolRamanand YadavNoch keine Bewertungen
- Passed 5104 13 21MELCS Baguio Roles of Theater EdtDokument89 SeitenPassed 5104 13 21MELCS Baguio Roles of Theater EdtChristopher David OlivaNoch keine Bewertungen
- 2014 GIA Education CatalogDokument56 Seiten2014 GIA Education Catalogtino3528Noch keine Bewertungen
- ENG8 - Q2 - Mod5 Compare and Contrast The Presentation of The Same Topic in Different Multimodal Texts Grace ManuelDokument11 SeitenENG8 - Q2 - Mod5 Compare and Contrast The Presentation of The Same Topic in Different Multimodal Texts Grace ManuelFreddy MarsucNoch keine Bewertungen
- Rancangan Pengajaran Harian Sains Kanak-Kanak Pendidikan KhasDokument2 SeitenRancangan Pengajaran Harian Sains Kanak-Kanak Pendidikan KhasnadiaburnNoch keine Bewertungen
- List of IFS Officers - 2015 As On Ifs Website-29.5.15Dokument370 SeitenList of IFS Officers - 2015 As On Ifs Website-29.5.15Mukesh Kumar100% (1)
- Caps Afrikaans Fal GR 1-3Dokument106 SeitenCaps Afrikaans Fal GR 1-3Louise SeptemberNoch keine Bewertungen
- Aqa Sociology Unit 4 June 11 Question PaperDokument8 SeitenAqa Sociology Unit 4 June 11 Question PaperGerardo PrattNoch keine Bewertungen
- Dll-Week12-Creative WritingDokument4 SeitenDll-Week12-Creative WritingCarna San JoseNoch keine Bewertungen
- CBSE Mid Term Exam InstructionsDokument1 SeiteCBSE Mid Term Exam InstructionsSamNoch keine Bewertungen
- QF EheaDokument200 SeitenQF Eheajose_dias_58Noch keine Bewertungen
- Significance of The Study & Acknowledgement and DedicationDokument9 SeitenSignificance of The Study & Acknowledgement and DedicationNiño Rovic Jimenez MagoNoch keine Bewertungen
- HandwashingDokument2 SeitenHandwashingBonita MendozaNoch keine Bewertungen
- Lesson 9 Pilot TestingDokument2 SeitenLesson 9 Pilot Testingclara dupitasNoch keine Bewertungen
- Psumt Newsletter FallDokument3 SeitenPsumt Newsletter Fallapi-251592269Noch keine Bewertungen
- كل ملفات طرق التدريسDokument689 Seitenكل ملفات طرق التدريسHesham RadwanNoch keine Bewertungen
- Downs & Wardle WritinDokument33 SeitenDowns & Wardle WritingpinqueNoch keine Bewertungen