Das könnte Ihnen auch gefallen
- Treatment of Perforating Internal Root Resorption With MTA: A Case ReportDokument5 SeitenTreatment of Perforating Internal Root Resorption With MTA: A Case ReportvishalbalpandeNoch keine Bewertungen
- Combined Therapy With Mineral Trioxide ADokument5 SeitenCombined Therapy With Mineral Trioxide AMihaela TuculinaNoch keine Bewertungen
- 2019 v13n4 008Dokument5 Seiten2019 v13n4 008Hanh LeNoch keine Bewertungen
- Clinical Study: A Liquid Membrane As A Barrier Membrane For Guided Bone RegenerationDokument6 SeitenClinical Study: A Liquid Membrane As A Barrier Membrane For Guided Bone RegenerationStanislav ȘuiuNoch keine Bewertungen
- Emdogain Research: Emdogain in Regenerative Periodontal Therapy. A Review of The LiteratureDokument4 SeitenEmdogain Research: Emdogain in Regenerative Periodontal Therapy. A Review of The LiteratureMohammed NabeelNoch keine Bewertungen
- Emdogain Research PDFDokument4 SeitenEmdogain Research PDFMohammed NabeelNoch keine Bewertungen
- Repair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingDokument8 SeitenRepair Processes of Experimental Root Fractures in Rat Molars Examined by Histopathological Techniques and 3D Micro-CT ImagingAhmad Ulil AlbabNoch keine Bewertungen
- Zybutz 2000Dokument10 SeitenZybutz 2000NareshNoch keine Bewertungen
- Untitled 3Dokument10 SeitenUntitled 3Satya AsatyaNoch keine Bewertungen
- Treatment of Abscessed Primary Molars Utilizing Lesion Sterilization and Tissue Repair: Literature Review and Report of Three CasesDokument14 SeitenTreatment of Abscessed Primary Molars Utilizing Lesion Sterilization and Tissue Repair: Literature Review and Report of Three CasesAsriNoch keine Bewertungen
- Micro Comparison With MacroDokument7 SeitenMicro Comparison With MacroDr. DeeptiNoch keine Bewertungen
- 3mix MPDokument6 Seiten3mix MPFirma Nurdinia DewiNoch keine Bewertungen
- Restoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationDokument5 SeitenRestoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationIntelligentiaNoch keine Bewertungen
- Surgical Management of Periapical Lesion Inmaxillary Incisorswith Combined Bone Graft and Platelet - Rich Fibrin: A Case ReportDokument5 SeitenSurgical Management of Periapical Lesion Inmaxillary Incisorswith Combined Bone Graft and Platelet - Rich Fibrin: A Case ReportTMDCH JournalNoch keine Bewertungen
- Van HeerdenDokument5 SeitenVan HeerdendorinkarakogluNoch keine Bewertungen
- Odontogenic Keratocyst Tumor: Report of Two CasesDokument6 SeitenOdontogenic Keratocyst Tumor: Report of Two CasesAnibal FuentesNoch keine Bewertungen
- JIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyDokument8 SeitenJIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyMedstudNoch keine Bewertungen
- IJOMS2007Dokument5 SeitenIJOMS2007api-3727708Noch keine Bewertungen
- An Innovative Technique To Restore The Non Vital Teeth With Wide Open Canals - A Clinical StudyDokument4 SeitenAn Innovative Technique To Restore The Non Vital Teeth With Wide Open Canals - A Clinical StudyIOSRjournalNoch keine Bewertungen
- Apioectomy Treatment FailingDokument6 SeitenApioectomy Treatment FailingMr-Ton DrgNoch keine Bewertungen
- Regenerative Pulp Therapy For Immature Non-Vital Tooth: A Case ReportDokument4 SeitenRegenerative Pulp Therapy For Immature Non-Vital Tooth: A Case ReportHansen WalaNoch keine Bewertungen
- Minimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityDokument7 SeitenMinimally Invasive Surgical Technique and Enamel Matrix Derivative in Intra-Bony Defects. I - Clinical Outcomes and MorbidityAnissa Citra UtamiNoch keine Bewertungen
- BIO C Repair With For Horizontal Root Fracture PDFDokument5 SeitenBIO C Repair With For Horizontal Root Fracture PDFDaniel Vivas0% (1)
- Densitometric Analysis of The Autogenous Demineralized Dentin Matrix On The Dental Socket Wound Healing Process in HumansDokument7 SeitenDensitometric Analysis of The Autogenous Demineralized Dentin Matrix On The Dental Socket Wound Healing Process in HumansTiago EscobarNoch keine Bewertungen
- Cortellini Et Al-2017-Journal of Clinical PeriodontologyDokument9 SeitenCortellini Et Al-2017-Journal of Clinical PeriodontologyCloudcynaraaNoch keine Bewertungen
- Ferrarotti Et Al. Journal of Clinical Periodontology (2018)Dokument10 SeitenFerrarotti Et Al. Journal of Clinical Periodontology (2018)Jose Luis Bladco MorenoNoch keine Bewertungen
- Dr. Neeraj AgrawalDokument4 SeitenDr. Neeraj AgrawalYulinda PrimilisaNoch keine Bewertungen
- Periodontal Parameters and Cervical Root Resorption During Orthodontic Tooh Movement - Giannopoulou2008Dokument6 SeitenPeriodontal Parameters and Cervical Root Resorption During Orthodontic Tooh Movement - Giannopoulou2008christian roblesNoch keine Bewertungen
- Guided BoneDokument6 SeitenGuided BonealeegaleanoNoch keine Bewertungen
- Pulpotomy With PRFDokument8 SeitenPulpotomy With PRFSai KalyanNoch keine Bewertungen
- Drughelp - Care 6.22Dokument10 SeitenDrughelp - Care 6.22Joko RifaiNoch keine Bewertungen
- Seehra2012 AJODO Retrospectivo MáscaraDokument6 SeitenSeehra2012 AJODO Retrospectivo MáscaraYeimi ArdilaNoch keine Bewertungen
- Coronectomy of The Mandibular Third MolarDokument2 SeitenCoronectomy of The Mandibular Third MolarChalu TamuraNoch keine Bewertungen
- RCT Comparing Implants With Turned and Anodically Oxidized Surfaces: A Pilot Study, A 3-Year Follow-UpDokument8 SeitenRCT Comparing Implants With Turned and Anodically Oxidized Surfaces: A Pilot Study, A 3-Year Follow-UpElena NicuNoch keine Bewertungen
- Healing 2020 MTA, PRFDokument8 SeitenHealing 2020 MTA, PRFMarwa Wagih ElboraeyNoch keine Bewertungen
- 227 235 SamamaDokument9 Seiten227 235 SamamayunitastyaningrumNoch keine Bewertungen
- DR Bhaumik Nanavati Proof ApprovedDokument6 SeitenDR Bhaumik Nanavati Proof ApprovedFahmi FirmansyahNoch keine Bewertungen
- Effects of Local Melatonin Application On Implant OsseointegrationDokument5 SeitenEffects of Local Melatonin Application On Implant OsseointegrationFrancisco VargasNoch keine Bewertungen
- J 1365-2591 2008 01474 XDokument10 SeitenJ 1365-2591 2008 01474 XNancyLiaoNoch keine Bewertungen
- Particularities in The Surgical Technique of Calvaria GraftDokument6 SeitenParticularities in The Surgical Technique of Calvaria Graftbalab2311Noch keine Bewertungen
- Reusing Dental Implants?: An Experimental Study For Detecting The Success Rates of Re-OsseointegrationDokument7 SeitenReusing Dental Implants?: An Experimental Study For Detecting The Success Rates of Re-OsseointegrationSatya AsatyaNoch keine Bewertungen
- 1 Three Years Follow Up of Combined Perio EndoDokument3 Seiten1 Three Years Follow Up of Combined Perio EndohanNoch keine Bewertungen
- Effects of Maxillary Protraction For Early Correction of Class IIIDokument7 SeitenEffects of Maxillary Protraction For Early Correction of Class IIIMariana SantosNoch keine Bewertungen
- Clin Oral Invest BTCP Type 1 Col ConesDokument10 SeitenClin Oral Invest BTCP Type 1 Col ConesPathivada LumbiniNoch keine Bewertungen
- Treatment Outcomes of Apexification or Revascularization in Nonvital Immature Permanent TeethDokument8 SeitenTreatment Outcomes of Apexification or Revascularization in Nonvital Immature Permanent Teeth吳國豪Noch keine Bewertungen
- 2022 AiutoDokument7 Seiten2022 AiutovivianaNoch keine Bewertungen
- Bone Reports: Case ReportDokument8 SeitenBone Reports: Case ReportDaniella NúñezNoch keine Bewertungen
- Regenerative Endodontic Treatment of A Traumatized Immature Necrotic Permanent Incisor - A Case Report - PMCDokument10 SeitenRegenerative Endodontic Treatment of A Traumatized Immature Necrotic Permanent Incisor - A Case Report - PMCbuch 453 gamerNoch keine Bewertungen
- RetrieveDokument10 SeitenRetrieveMaria CorenaNoch keine Bewertungen
- Clinical StudyDokument13 SeitenClinical StudyJuliana Gomes BarretoNoch keine Bewertungen
- Piezosurgery Vs ConventionalDokument5 SeitenPiezosurgery Vs ConventionalSaskia ParamitaNoch keine Bewertungen
- Micro-Computed Tomographic Analysis of Apical Foramen Enlargement of Mature Teeth: A Cadaveric StudyDokument6 SeitenMicro-Computed Tomographic Analysis of Apical Foramen Enlargement of Mature Teeth: A Cadaveric StudyJonatan VelezNoch keine Bewertungen
- The Positive Effect of Tenting Screws For Primary Horizontal Guided Bone Regeneration - A Retrospective Study Based On Cone-Beam Computed Tomography Data - Hämmerle 2020Dokument10 SeitenThe Positive Effect of Tenting Screws For Primary Horizontal Guided Bone Regeneration - A Retrospective Study Based On Cone-Beam Computed Tomography Data - Hämmerle 2020LEONARDO ALBERTO CRESPIN ZEPEDANoch keine Bewertungen
- Zuhr Et Al-2014-Journal of Clinical PeriodontologyDokument20 SeitenZuhr Et Al-2014-Journal of Clinical PeriodontologyAbad Salcedo100% (1)
- Delir 2013Dokument7 SeitenDelir 2013Karam EidNoch keine Bewertungen
- The Novel Periosteal Flap Stretch Technique: A Predictable Method To Achieve and Maintain Primary Closure in Augmentative ProceduresDokument10 SeitenThe Novel Periosteal Flap Stretch Technique: A Predictable Method To Achieve and Maintain Primary Closure in Augmentative ProceduresAshish PandaNoch keine Bewertungen
- Articulo 3Dokument9 SeitenArticulo 3Javier CastilloNoch keine Bewertungen
- Extraoral Prostheses Using Introral Implants PDFDokument6 SeitenExtraoral Prostheses Using Introral Implants PDFqueka555_5Noch keine Bewertungen
- Journal of Periodontology - 2022 - Monje - Significance of Barrier Membrane On The Reconstructive Therapy ofDokument13 SeitenJournal of Periodontology - 2022 - Monje - Significance of Barrier Membrane On The Reconstructive Therapy of安西 泰規Noch keine Bewertungen
- YTC Initial ChecklistDokument3 SeitenYTC Initial ChecklistBrian KohlerNoch keine Bewertungen
- Combine Each Pair of Sentences With The Conjunction in Parenthesis To Make A New SentenceDokument3 SeitenCombine Each Pair of Sentences With The Conjunction in Parenthesis To Make A New SentenceKranti PrajapatiNoch keine Bewertungen
- DTCE Weeks Oct 214 FNLDokument8 SeitenDTCE Weeks Oct 214 FNLKranti PrajapatiNoch keine Bewertungen
- Past TenseDokument6 SeitenPast TenseKranti PrajapatiNoch keine Bewertungen
- AB Amaris DR Marques Australasian Dentist June 2011Dokument3 SeitenAB Amaris DR Marques Australasian Dentist June 2011Kranti PrajapatiNoch keine Bewertungen
- (Ebook - Psychology) The World of Subconscious MindDokument315 Seiten(Ebook - Psychology) The World of Subconscious MindKranti PrajapatiNoch keine Bewertungen
- DtceDokument10 SeitenDtceKranti PrajapatiNoch keine Bewertungen
- Creating Well-Obturated Canals - The Use of Warm Vertical Condensation Techniques - Dentistry TodayDokument9 SeitenCreating Well-Obturated Canals - The Use of Warm Vertical Condensation Techniques - Dentistry TodayKranti PrajapatiNoch keine Bewertungen
- An Improved Quadrant Class II Composite Technique - Dentistry TodayDokument6 SeitenAn Improved Quadrant Class II Composite Technique - Dentistry TodayKranti PrajapatiNoch keine Bewertungen
- Advances in Biomechanical Preparation - Dentistry TodayDokument5 SeitenAdvances in Biomechanical Preparation - Dentistry TodayKranti PrajapatiNoch keine Bewertungen
- Clinical Applications - Apical Negative Pressure Irrigation - Dentistry TodayDokument7 SeitenClinical Applications - Apical Negative Pressure Irrigation - Dentistry TodayKranti PrajapatiNoch keine Bewertungen
- An Improved Glass Ionomer Restorative System - Stress-Bearing Class I and II Indications - Dentistry TodayDokument7 SeitenAn Improved Glass Ionomer Restorative System - Stress-Bearing Class I and II Indications - Dentistry TodayKranti PrajapatiNoch keine Bewertungen
- CBCT Imaging's Insight Into Endodontic Retreatment Success - Dentistry TodayDokument7 SeitenCBCT Imaging's Insight Into Endodontic Retreatment Success - Dentistry TodayKranti PrajapatiNoch keine Bewertungen
- Monetary Policy Securities Market 2074Dokument2 SeitenMonetary Policy Securities Market 2074Kranti PrajapatiNoch keine Bewertungen
- 1 s2.0 S0011853213000347 MainDokument15 Seiten1 s2.0 S0011853213000347 MainKranti PrajapatiNoch keine Bewertungen
- Monetary Policy Securities Market 2074Dokument2 SeitenMonetary Policy Securities Market 2074Kranti PrajapatiNoch keine Bewertungen
- Dental Clinics of North America Use of Portable Monitoring For Sleep Disordered Breathing Treated With An Oral Appliance 445 452Dokument8 SeitenDental Clinics of North America Use of Portable Monitoring For Sleep Disordered Breathing Treated With An Oral Appliance 445 452Kranti PrajapatiNoch keine Bewertungen
- Dental Clinics of North America Medical Disorders Impacted by Obstructive Sleep Apnea 373 386Dokument14 SeitenDental Clinics of North America Medical Disorders Impacted by Obstructive Sleep Apnea 373 386Kranti PrajapatiNoch keine Bewertungen
- 1 s2.0 S0011853213000438 MainDokument2 Seiten1 s2.0 S0011853213000438 MainKranti PrajapatiNoch keine Bewertungen
- Dental Clinics of North America Sleep Medicine in Dentistry Xi XiiiDokument3 SeitenDental Clinics of North America Sleep Medicine in Dentistry Xi XiiiKranti PrajapatiNoch keine Bewertungen
- Dental Clinics of North America Appendix 485 486Dokument2 SeitenDental Clinics of North America Appendix 485 486Kranti PrajapatiNoch keine Bewertungen
- Preface: Scott S. de Rossi, DMD David A. Sirois, DMD, PHD EditorsDokument2 SeitenPreface: Scott S. de Rossi, DMD David A. Sirois, DMD, PHD EditorsKranti PrajapatiNoch keine Bewertungen
- Diagnostic Imaging For Temporomandibular Disorders and Orofacial Pain 2013 Dental Clinics of North AmericaDokument14 SeitenDiagnostic Imaging For Temporomandibular Disorders and Orofacial Pain 2013 Dental Clinics of North AmericaazizNoch keine Bewertungen
- 1 s2.0 S0011853213000438 MainDokument2 Seiten1 s2.0 S0011853213000438 MainKranti PrajapatiNoch keine Bewertungen
- Trushkowsky - 2011 - Dental Clinics of North America PDFDokument10 SeitenTrushkowsky - 2011 - Dental Clinics of North America PDFKranti PrajapatiNoch keine Bewertungen
- Preface Oralandcraniofacialimplant Reconstructionasfoundation ForrestorativedentistryDokument1 SeitePreface Oralandcraniofacialimplant Reconstructionasfoundation ForrestorativedentistryKranti PrajapatiNoch keine Bewertungen
- Erratum IxDokument3 SeitenErratum IxKranti PrajapatiNoch keine Bewertungen
- 1 s2.0 S001185321300030X MainDokument27 Seiten1 s2.0 S001185321300030X MainKranti PrajapatiNoch keine Bewertungen
- Bonnick - 2011 - Dental Clinics of North America PDFDokument14 SeitenBonnick - 2011 - Dental Clinics of North America PDFKranti PrajapatiNoch keine Bewertungen
- 2011 4 PDFDokument23 Seiten2011 4 PDFKranti PrajapatiNoch keine Bewertungen
- Astm 2017-F2059Dokument5 SeitenAstm 2017-F2059laythNoch keine Bewertungen
- L2 Biostatistics ProbabilityDokument84 SeitenL2 Biostatistics ProbabilityAaron CiudadNoch keine Bewertungen
- Armor MagazineDokument32 SeitenArmor Magazine"Rufus"100% (1)
- LPG GasDokument39 SeitenLPG Gasv prasanthNoch keine Bewertungen
- Poems Prescribed For 2012-2014 English B CSEC ExamsDokument24 SeitenPoems Prescribed For 2012-2014 English B CSEC ExamsJorge Martinez Sr.100% (2)
- VTA28-G5: Fuel OptimizedDokument3 SeitenVTA28-G5: Fuel OptimizedIslam HemdanNoch keine Bewertungen
- Sheet Metal Manufacturing Companies NoidaDokument9 SeitenSheet Metal Manufacturing Companies NoidaAmanda HoldenNoch keine Bewertungen
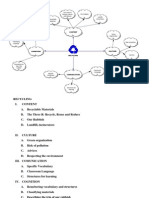
- Recycling Mind MapDokument2 SeitenRecycling Mind Mapmsole124100% (1)
- Ge Fairchild Brochure PDFDokument2 SeitenGe Fairchild Brochure PDFDharmesh patelNoch keine Bewertungen
- Egt Margen From The Best ArticalDokument6 SeitenEgt Margen From The Best ArticalakeelNoch keine Bewertungen
- Plato: Epistemology: Nicholas WhiteDokument2 SeitenPlato: Epistemology: Nicholas WhiteAnonymous HCqIYNvNoch keine Bewertungen
- Time Value of Money LectureDokument54 SeitenTime Value of Money LectureRanin, Manilac Melissa SNoch keine Bewertungen
- L GH Catalog PullingDokument60 SeitenL GH Catalog PullingLuis LuperdiNoch keine Bewertungen
- History and Philo of ScienceDokument5 SeitenHistory and Philo of ScienceJan Oliver YaresNoch keine Bewertungen
- Contact Inform 2002 PDFDokument24 SeitenContact Inform 2002 PDFFrank AlmeidaNoch keine Bewertungen
- Stanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)Dokument308 SeitenStanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)georgemultiplusNoch keine Bewertungen
- BECO UACE Chem2Dokument6 SeitenBECO UACE Chem2EMMANUEL BIRUNGINoch keine Bewertungen
- Dialog Bahasa InggirsDokument2 SeitenDialog Bahasa InggirsKeRtha NeghaRaNoch keine Bewertungen
- Shell Gadus: Designed To Do More. Just Like Our Greases - Shell GadusDokument2 SeitenShell Gadus: Designed To Do More. Just Like Our Greases - Shell Gadusperi irawanNoch keine Bewertungen
- Leadership Games and ActivitiesDokument38 SeitenLeadership Games and ActivitiesWilliam Oliss100% (1)
- Motor CAT C13 AcertDokument3 SeitenMotor CAT C13 AcertJosé Gonzalez100% (4)
- Thermoplastic Tubing: Catalogue 5210/UKDokument15 SeitenThermoplastic Tubing: Catalogue 5210/UKGeo BuzatuNoch keine Bewertungen
- Kwasaki ZX10R 16Dokument101 SeitenKwasaki ZX10R 16OliverNoch keine Bewertungen
- The Wild T1 TheodoliteDokument61 SeitenThe Wild T1 TheodoliteCJLara100% (1)
- 39ED3050CT - RT49S - AP Service ManualDokument31 Seiten39ED3050CT - RT49S - AP Service Manualبوند بوند100% (1)
- Furuno CA 400Dokument345 SeitenFuruno CA 400Димон100% (3)
- Sketchup-Rhino Cheat SheetDokument1 SeiteSketchup-Rhino Cheat Sheetxanext7Noch keine Bewertungen
- A Textual Introduction To Acarya Vasuvan PDFDokument3 SeitenA Textual Introduction To Acarya Vasuvan PDFJim LeeNoch keine Bewertungen
- Kuiz1 210114Dokument12 SeitenKuiz1 210114Vincent HoNoch keine Bewertungen
- Easergy PS100 48VDC Power SupplyDokument2 SeitenEasergy PS100 48VDC Power SupplyRichard SyNoch keine Bewertungen