Das könnte Ihnen auch gefallen
- Mastoid Abscess in Acute and Chronic Otitis Media: Original ArticleDokument7 SeitenMastoid Abscess in Acute and Chronic Otitis Media: Original ArticleChin Edward ChandraNoch keine Bewertungen
- Mastoiditis PDFDokument4 SeitenMastoiditis PDFMildred MontNoch keine Bewertungen
- Acute Mastoiditis in Children As Persisting ProblemDokument5 SeitenAcute Mastoiditis in Children As Persisting ProblemRafael BagusNoch keine Bewertungen
- Pi Is 2090074012000357Dokument6 SeitenPi Is 2090074012000357Diggi VioNoch keine Bewertungen
- Otitie Media Adhesiva JMCM - Volume 9 - Issue 1 - Pages 108-112Dokument5 SeitenOtitie Media Adhesiva JMCM - Volume 9 - Issue 1 - Pages 108-112Teuku Ahmad HasanyNoch keine Bewertungen
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDokument5 SeitenPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007Noch keine Bewertungen
- Malignant Otitis External-Our Experience: R. B. Sardesai, T. KrishnakumarDokument4 SeitenMalignant Otitis External-Our Experience: R. B. Sardesai, T. KrishnakumarSuci PramadianiNoch keine Bewertungen
- Management of Acute Mastoiditis in Children. A Retrospective Study and Literature ReviewDokument5 SeitenManagement of Acute Mastoiditis in Children. A Retrospective Study and Literature ReviewAnonymous QPXAgjBwNoch keine Bewertungen
- Differences Between Children and Adults With Otitis Media With Effusion Treated With CO Laser MyringotomyDokument7 SeitenDifferences Between Children and Adults With Otitis Media With Effusion Treated With CO Laser MyringotomyIndra PratamaNoch keine Bewertungen
- Jurnal Reading OtomikosisDokument4 SeitenJurnal Reading OtomikosisTria JuwitaNoch keine Bewertungen
- Otogenic Brain Abscess Our ExperienceDokument5 SeitenOtogenic Brain Abscess Our ExperienceNeysaAzaliaEfrimaisaNoch keine Bewertungen
- 2018 Article 1362 PDFDokument5 Seiten2018 Article 1362 PDFAuliaMahdaniatiNoch keine Bewertungen
- C CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TDokument7 SeitenC CA AS SC CL Liin Niiq QU UE E // C CA AS SE ER RE EP PO OR RT TG Virucha Meivila IINoch keine Bewertungen
- Complications of Suppurative Otitis Media: Still A Problem in The 21st CenturyDokument7 SeitenComplications of Suppurative Otitis Media: Still A Problem in The 21st CenturyNisa SulistiaNoch keine Bewertungen
- Management of Paediatric Acute Mastoiditis: Systematic ReviewDokument9 SeitenManagement of Paediatric Acute Mastoiditis: Systematic ReviewAldy GeriNoch keine Bewertungen
- Anestesia en Labio LeporinoDokument5 SeitenAnestesia en Labio LeporinoYosset Emilet Rodrìguez CalderònNoch keine Bewertungen
- Management of Necrotizing Otitis Externa: Our Experience With Forty-Three PatientsDokument5 SeitenManagement of Necrotizing Otitis Externa: Our Experience With Forty-Three Patientsmenik ayuNoch keine Bewertungen
- Updated Management Strategies For Mastoiditis and PDFDokument7 SeitenUpdated Management Strategies For Mastoiditis and PDFJr SparkNoch keine Bewertungen
- Updated Management Strategies For Mastoiditis and Mastoid AbscessDokument6 SeitenUpdated Management Strategies For Mastoiditis and Mastoid AbscessRonnyPujaKusumaNoch keine Bewertungen
- Emergency Medicine:: Pediatric Deep Neck Space Abscesses: A Prospective Observational StudyDokument6 SeitenEmergency Medicine:: Pediatric Deep Neck Space Abscesses: A Prospective Observational StudyG Virucha Meivila IINoch keine Bewertungen
- Ramsay Hunt SyndromeDokument4 SeitenRamsay Hunt SyndromeRiadhus Machfud AlfianNoch keine Bewertungen
- Otogenic Complications of Otitis Media Experience at Tertiary Care HospitalDokument5 SeitenOtogenic Complications of Otitis Media Experience at Tertiary Care HospitalAjeng Ratna HaryantiNoch keine Bewertungen
- 1 s2.0 S0165587617302975 Main PDFDokument4 Seiten1 s2.0 S0165587617302975 Main PDFAchmad YunusNoch keine Bewertungen
- 2012 VideoDokument4 Seiten2012 VideoNur LaelaNoch keine Bewertungen
- Oral Cortcisosteroid PulseDokument10 SeitenOral Cortcisosteroid PulseVilt VilNoch keine Bewertungen
- Deep Neck Infections: Continuing Burden in Developing World: Original ArticleDokument4 SeitenDeep Neck Infections: Continuing Burden in Developing World: Original ArticlevaNoch keine Bewertungen
- Invasive Sino-Aspergillosis in ImmunocompetentDokument5 SeitenInvasive Sino-Aspergillosis in Immunocompetentabeer alrofaeyNoch keine Bewertungen
- Management of Paediatric Acute Mastoiditis Systematic ReviewDokument9 SeitenManagement of Paediatric Acute Mastoiditis Systematic Reviewteu.yamNoch keine Bewertungen
- Tubercular Otitis Media: Demystifying Its Nuances and An Update On The Tenets of Emerging PerspectivesDokument9 SeitenTubercular Otitis Media: Demystifying Its Nuances and An Update On The Tenets of Emerging PerspectivesAditya HendraNoch keine Bewertungen
- Ijced 21 004Dokument7 SeitenIjced 21 004Eduardo Jesús Núñez JordánNoch keine Bewertungen
- Treatment of Serous Otitis Media: D.T. Orishchak, N.V. Vasyliuk, O.R. Orishchak, H.V. Khrebtiuk, R.M. FishchukDokument2 SeitenTreatment of Serous Otitis Media: D.T. Orishchak, N.V. Vasyliuk, O.R. Orishchak, H.V. Khrebtiuk, R.M. Fishchukgemala wahabNoch keine Bewertungen
- Celulitis PeriorbitariaDokument4 SeitenCelulitis PeriorbitariaJose Carlos Guerra RangelNoch keine Bewertungen
- Jced 9 E319Dokument6 SeitenJced 9 E319sorayahyuraNoch keine Bewertungen
- Comparison of Limberg Flep and Adipofacial Flep in The Surgical Treatment of Pilonidal Sinus A Prospective Randomized Clinical StudyDokument5 SeitenComparison of Limberg Flep and Adipofacial Flep in The Surgical Treatment of Pilonidal Sinus A Prospective Randomized Clinical StudyAthenaeum Scientific PublishersNoch keine Bewertungen
- JurnallDokument27 SeitenJurnallMelan JustariNoch keine Bewertungen
- Miiringotomi OMEDokument7 SeitenMiiringotomi OMEamaliaNoch keine Bewertungen
- Mucormycosis of The Hard Palate A Case ReportDokument3 SeitenMucormycosis of The Hard Palate A Case ReportrgumralNoch keine Bewertungen
- Otomycosis Clinical Features, Predisposing Factors and Treatment ImplicationsDokument4 SeitenOtomycosis Clinical Features, Predisposing Factors and Treatment ImplicationsMortezaNoch keine Bewertungen
- ZBJQS8 Yk 5 KDQ 7 QF VBF 9 LVW LDokument9 SeitenZBJQS8 Yk 5 KDQ 7 QF VBF 9 LVW LJoão Rafael Gomes de LunaNoch keine Bewertungen
- 21 2019 PDFDokument4 Seiten21 2019 PDFNajam IqbalNoch keine Bewertungen
- Clinical and Pathologic Analyses of Tuberculosis in The Oral Cavity: Report of 11 CasesDokument8 SeitenClinical and Pathologic Analyses of Tuberculosis in The Oral Cavity: Report of 11 CasesMaria Lozano Figueroa 5to secNoch keine Bewertungen
- Original Article: Wasif Siddique, Abdul Hakeem, Kamran Ashfaq, Maryam Khan, Asif Alam GulDokument5 SeitenOriginal Article: Wasif Siddique, Abdul Hakeem, Kamran Ashfaq, Maryam Khan, Asif Alam GulGalvin GiffariNoch keine Bewertungen
- Infection of Impacted Lower ThirdDokument5 SeitenInfection of Impacted Lower ThirdjoseluisNoch keine Bewertungen
- Omsk 1 PDFDokument4 SeitenOmsk 1 PDFtarikhNoch keine Bewertungen
- Endoscopic Sinus Surgery: Indications and Complications: February 2020Dokument7 SeitenEndoscopic Sinus Surgery: Indications and Complications: February 2020husnul khatimahNoch keine Bewertungen
- Jurnal+oma+dr+muslim+sp THT-KLDokument6 SeitenJurnal+oma+dr+muslim+sp THT-KLHesti RiksawatiNoch keine Bewertungen
- Heim 2017Dokument13 SeitenHeim 2017Muhamad SaifuddinNoch keine Bewertungen
- 1191 4833 2 PBDokument6 Seiten1191 4833 2 PBWilson WibisonoNoch keine Bewertungen
- Pe Rich On DR It Is of The Auricle and Its ManagementDokument6 SeitenPe Rich On DR It Is of The Auricle and Its ManagementmitaNoch keine Bewertungen
- Chiapas Co 1995Dokument5 SeitenChiapas Co 1995Juan Augusto Fernández TarazonaNoch keine Bewertungen
- Jurnal PatogenesisDokument6 SeitenJurnal PatogenesisErmiati EmhyNoch keine Bewertungen
- Ijoto2017 9650910 PDFDokument7 SeitenIjoto2017 9650910 PDFSeptia P. MayasariNoch keine Bewertungen
- Sphenoid Sinus Diseases - A Review of 1,442 PatientsDokument8 SeitenSphenoid Sinus Diseases - A Review of 1,442 PatientsMario NarváezNoch keine Bewertungen
- A Comprehensive Study of Intestinal ObstructionDokument9 SeitenA Comprehensive Study of Intestinal ObstructionRoxana ElenaNoch keine Bewertungen
- Preseptal and Orbital Cellulitis: A 10-Year Review of Hospitalized PatientsDokument8 SeitenPreseptal and Orbital Cellulitis: A 10-Year Review of Hospitalized PatientsApril MitchellNoch keine Bewertungen
- The Course of Dry Eye After Phacoemulsification Surgery: Researcharticle Open AccessDokument5 SeitenThe Course of Dry Eye After Phacoemulsification Surgery: Researcharticle Open AccessDestia AnandaNoch keine Bewertungen
- SJAMS 66 2563 2566 C PDFDokument4 SeitenSJAMS 66 2563 2566 C PDFVitta Kusma WijayaNoch keine Bewertungen
- Ghanie Irwan 2019 J. Phys.: Conf. Ser. 1246 012019Dokument9 SeitenGhanie Irwan 2019 J. Phys.: Conf. Ser. 1246 012019mellysa iskandarNoch keine Bewertungen
- Risk AssessmentDokument2 SeitenRisk Assessmentapi-551545059Noch keine Bewertungen
- Sexual HealthDokument11 SeitenSexual Healthapi-236516264Noch keine Bewertungen
- Insomnia PatternsDokument10 SeitenInsomnia PatternsRNoch keine Bewertungen
- Module 1 Overview of Biosafety LevelsDokument33 SeitenModule 1 Overview of Biosafety LevelsSara Belayineh100% (2)
- California School Immunization RecordDokument2 SeitenCalifornia School Immunization RecordJeevitha RoyapathiNoch keine Bewertungen
- Respiratory Support in ChildDokument8 SeitenRespiratory Support in ChildHưng TrầnNoch keine Bewertungen
- Klasifikasi Dan DD MigrenDokument17 SeitenKlasifikasi Dan DD MigrenYosephinNoch keine Bewertungen
- SECOND YEAR PHARMD Syllabus PU PDFDokument14 SeitenSECOND YEAR PHARMD Syllabus PU PDFRIYA ROYNoch keine Bewertungen
- Sfsac@xmu - Edu.my: To: From: FIS1012050@. Xmu - Edu.my Subject: Concern of Final Examination Amid Covid-19Dokument2 SeitenSfsac@xmu - Edu.my: To: From: FIS1012050@. Xmu - Edu.my Subject: Concern of Final Examination Amid Covid-19Ahmad RazaNoch keine Bewertungen
- Cowden S Disease A Rare Cause of Oral Sis 2002 Journal of Laryngology and OtologyDokument3 SeitenCowden S Disease A Rare Cause of Oral Sis 2002 Journal of Laryngology and Otologydasea01Noch keine Bewertungen
- DRNB Medical Gastroenterology Paper1Dokument4 SeitenDRNB Medical Gastroenterology Paper1Srinivas PingaliNoch keine Bewertungen
- Newsletter: WHO PharmaceuticalsDokument27 SeitenNewsletter: WHO PharmaceuticalsGammachuu Leejjiisa Mul'ataa SabbooqaaNoch keine Bewertungen
- Classical Western FormulasDokument4 SeitenClassical Western FormulasSofia MirandaNoch keine Bewertungen
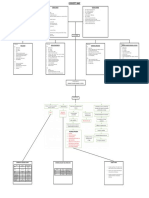
- IM-CAP Concept MapDokument1 SeiteIM-CAP Concept MapTrisNoch keine Bewertungen
- Descriptive Research Regarding The COVID-19Dokument5 SeitenDescriptive Research Regarding The COVID-19Mish Lei FranxhNoch keine Bewertungen
- Clinical Practice Guidelines 2021 - Egyptian ORL Society... - Copy-1-185Dokument185 SeitenClinical Practice Guidelines 2021 - Egyptian ORL Society... - Copy-1-185abdalla materNoch keine Bewertungen
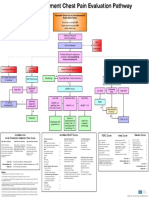
- Emergency Department Chest Pain Evaluation PathwayDokument2 SeitenEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNoch keine Bewertungen
- Presentation Classification and Segmentation of TuberculosisDokument3 SeitenPresentation Classification and Segmentation of Tuberculosissaissi1701Noch keine Bewertungen
- Sulfur Sticks SDS 05-2016 IRPLLC Rev3Dokument3 SeitenSulfur Sticks SDS 05-2016 IRPLLC Rev3juan leyyonNoch keine Bewertungen
- NCP GastroenteritisDokument1 SeiteNCP GastroenteritisFranchesca PaunganNoch keine Bewertungen
- 2.1 NCM 109 - Pregestational ConditionsDokument6 Seiten2.1 NCM 109 - Pregestational ConditionsSittie Haneen TabaraNoch keine Bewertungen
- Cherry Eye: Prolapse of Third Eyelid Gland in Dog-A Case ReportDokument4 SeitenCherry Eye: Prolapse of Third Eyelid Gland in Dog-A Case ReportRocioNoch keine Bewertungen
- ChleraDokument26 SeitenChleraadelekeyusufNoch keine Bewertungen
- SplenectomyDokument5 SeitenSplenectomysharjil chaudhryNoch keine Bewertungen
- OphthalmologyDokument24 SeitenOphthalmologyJessica McCroryNoch keine Bewertungen
- DX StdieDokument22 SeitenDX Stdietimie_reyesNoch keine Bewertungen
- Central Nervous System StimulantsDokument6 SeitenCentral Nervous System StimulantsNathalia CabalseNoch keine Bewertungen
- Case PresentationDokument14 SeitenCase PresentationFatema RavatNoch keine Bewertungen
- Yoga and MeditationDokument28 SeitenYoga and MeditationVivek VashisthNoch keine Bewertungen