Das könnte Ihnen auch gefallen
- Obs History MandarinDokument1 SeiteObs History MandarinHo Yong WaiNoch keine Bewertungen
- Dengue CaseDokument4 SeitenDengue CaseHo Yong WaiNoch keine Bewertungen
- Dengue CaseDokument4 SeitenDengue CaseHo Yong WaiNoch keine Bewertungen
- Dengue CaseDokument4 SeitenDengue CaseHo Yong WaiNoch keine Bewertungen
- Cerebellar SyndromeDokument2 SeitenCerebellar SyndromeHo Yong WaiNoch keine Bewertungen
- Approach To The Patient With Dysphagia PDFDokument7 SeitenApproach To The Patient With Dysphagia PDFHo Yong Wai100% (1)
- Approach To The Patient With Dysphagia PDFDokument7 SeitenApproach To The Patient With Dysphagia PDFHo Yong Wai100% (1)
- Department Coordinator BioDokument1 SeiteDepartment Coordinator BioHo Yong WaiNoch keine Bewertungen
- Bipolar DisorderDokument1 SeiteBipolar DisorderHo Yong WaiNoch keine Bewertungen
- HivDokument1 SeiteHivHo Yong WaiNoch keine Bewertungen
- Paediatrics at A GlanceDokument2 SeitenPaediatrics at A GlanceHo Yong WaiNoch keine Bewertungen
- Taking A Gynaecological HistoryDokument21 SeitenTaking A Gynaecological Historyasif_siddiqui_2100% (1)
- Ob-Gyn Clinical Cases (From Apgo Site)Dokument221 SeitenOb-Gyn Clinical Cases (From Apgo Site)jamieNoch keine Bewertungen
- Part 1Dokument18 SeitenPart 1Ho Yong WaiNoch keine Bewertungen
- Common Long Cases IM Sem 7Dokument3 SeitenCommon Long Cases IM Sem 7Ho Yong WaiNoch keine Bewertungen
- Reflective ReportDokument2 SeitenReflective ReportHo Yong WaiNoch keine Bewertungen
- Common ENT ComplaintsDokument9 SeitenCommon ENT ComplaintsHo Yong WaiNoch keine Bewertungen
- BVMDokument3 SeitenBVMHo Yong WaiNoch keine Bewertungen
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Dokument68 SeitenCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1Noch keine Bewertungen
- HomeworkDokument12 SeitenHomeworkHo Yong WaiNoch keine Bewertungen
- Lesson 3 ReviewDokument4 SeitenLesson 3 ReviewHo Yong WaiNoch keine Bewertungen
- Internal Medicine Venepuncture IM & SC Injection Cannulation ABGDokument1 SeiteInternal Medicine Venepuncture IM & SC Injection Cannulation ABGHo Yong WaiNoch keine Bewertungen
- Lesson 6 ReviewDokument2 SeitenLesson 6 ReviewHo Yong WaiNoch keine Bewertungen
- Lesson 9 ReviewDokument2 SeitenLesson 9 ReviewHo Yong WaiNoch keine Bewertungen
- TBL RheumatologyDokument16 SeitenTBL RheumatologyHo Yong WaiNoch keine Bewertungen
- Lesson 8 ReviewDokument3 SeitenLesson 8 ReviewHo Yong WaiNoch keine Bewertungen
- Lesson 5 ReviewDokument4 SeitenLesson 5 ReviewHo Yong WaiNoch keine Bewertungen
- TBL PaedsDokument10 SeitenTBL PaedsHo Yong WaiNoch keine Bewertungen
- Psy Case DiscussionDokument16 SeitenPsy Case DiscussionHo Yong WaiNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 1 Introduction Clinical Pharmacy 2Dokument54 Seiten1 Introduction Clinical Pharmacy 2Sajid Hassan GhafoorNoch keine Bewertungen
- Final 2019 Mue Report Vancomycin CTR With GraphsDokument6 SeitenFinal 2019 Mue Report Vancomycin CTR With Graphsapi-493355126Noch keine Bewertungen
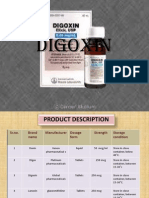
- DigoxinDokument20 SeitenDigoxinAbdulRehmanChaudaryNoch keine Bewertungen
- Stevens-Johnson Syndrome Triggered by A Combination of Clobazam, Lamotrigine and Valproic Acid in A 7-Year-Old ChildDokument6 SeitenStevens-Johnson Syndrome Triggered by A Combination of Clobazam, Lamotrigine and Valproic Acid in A 7-Year-Old ChildFARMASIRSUMAMPANGNoch keine Bewertungen
- Spot 2023 Brochure - FinalDokument3 SeitenSpot 2023 Brochure - FinalMontesqieu SilalahiNoch keine Bewertungen
- Piroxicam StudyDokument4 SeitenPiroxicam StudyRishabh SarawagiNoch keine Bewertungen
- Adrenergic DrugsDokument10 SeitenAdrenergic DrugsMr VoralpenNoch keine Bewertungen
- Pharmaceuticals For Small Animal Internal MedicineDokument11 SeitenPharmaceuticals For Small Animal Internal Medicineahmet öztürkNoch keine Bewertungen
- Dispensing AnsDokument197 SeitenDispensing AnsPrincess Ronsable100% (1)
- Comparison of Double-Flap Incision To Periosteal Releasing Incision For Flap AdvancementDokument8 SeitenComparison of Double-Flap Incision To Periosteal Releasing Incision For Flap AdvancementAnthony LiNoch keine Bewertungen
- Valsartan Recall: Angiotensin Ii Receptor Blockers (Arbs) Equivalent DosingDokument2 SeitenValsartan Recall: Angiotensin Ii Receptor Blockers (Arbs) Equivalent DosingGlory Claudia KarundengNoch keine Bewertungen
- Tranexamic Acid Drug StudyDokument3 SeitenTranexamic Acid Drug Studyswitchlers anneNoch keine Bewertungen
- Polygynax Vaginal CapsuleDokument4 SeitenPolygynax Vaginal Capsuleemmanuelquaye846Noch keine Bewertungen
- Antifungal Drugs: Dr:Samah AlshygiDokument19 SeitenAntifungal Drugs: Dr:Samah AlshygiKhan Khan100% (1)
- The New Advanced Cardiac Life Support GuidelinesDokument52 SeitenThe New Advanced Cardiac Life Support GuidelinesFandy Hazzy AlfataNoch keine Bewertungen
- FArmasi RS Dan Klinik KomprehensifDokument8 SeitenFArmasi RS Dan Klinik Komprehensifklinik dktNoch keine Bewertungen
- Electro Convulsive Therapy APADokument214 SeitenElectro Convulsive Therapy APAastral055356Noch keine Bewertungen
- Pacu Tylenol PresentationDokument10 SeitenPacu Tylenol PresentationStanford AnesthesiaNoch keine Bewertungen
- Placida Plus 0.5 Mg10 MG Tablet - Uses, Side Effects, Substitutes, Composition and More LybrateDokument1 SeitePlacida Plus 0.5 Mg10 MG Tablet - Uses, Side Effects, Substitutes, Composition and More LybrateJuzer SongerwalaNoch keine Bewertungen
- Prelim (Drug Delivery System)Dokument133 SeitenPrelim (Drug Delivery System)Vanessa DL100% (1)
- Research On The Different Pharmacy Setting of Other ASEAN CountriesDokument11 SeitenResearch On The Different Pharmacy Setting of Other ASEAN CountriesAngel Rose GeraldeNoch keine Bewertungen
- Annisa Fitriani-19.008-THE TASK OF MAKING SENTENCESDokument2 SeitenAnnisa Fitriani-19.008-THE TASK OF MAKING SENTENCESAnnisa FitrianiNoch keine Bewertungen
- Exam MarchDokument2 SeitenExam MarchkathlynmangasiNoch keine Bewertungen
- Mag NMM022009Dokument60 SeitenMag NMM022009DanceportugalNoch keine Bewertungen
- Neuromuscular Blocking DrugsDokument5 SeitenNeuromuscular Blocking DrugsTherese Jane TiradorNoch keine Bewertungen
- Daftar Obat: InjeksiDokument3 SeitenDaftar Obat: InjeksiDolsky MessiNoch keine Bewertungen
- Name of Pharmacy: ................................. CityDokument1 SeiteName of Pharmacy: ................................. Cityravi sheladiyaNoch keine Bewertungen
- Claris Life SciencesDokument20 SeitenClaris Life Sciencesten_ishan88Noch keine Bewertungen
- Laporan Penggunaan Februari 2022Dokument7 SeitenLaporan Penggunaan Februari 2022Rara LaveniaNoch keine Bewertungen
- Clinical ToxicologyDokument79 SeitenClinical ToxicologySaddam HossainNoch keine Bewertungen