Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Wound Care PDFDokument100 SeitenWound Care PDFVanessaMUeller100% (2)
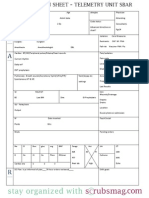
- Nurse Brain Sheet Telemetry Unit SBARDokument1 SeiteNurse Brain Sheet Telemetry Unit SBARvsosa624Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Nurse Brain Sheet With Shift HoursDokument2 SeitenNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Nclex Past QuestionsDokument452 SeitenNclex Past Questionsjyka100% (21)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Nurse Brain Sheet Half SizeDokument1 SeiteNurse Brain Sheet Half Sizevsosa624Noch keine Bewertungen
- Lab Values Chart GuideDokument5 SeitenLab Values Chart GuideVanessaMUeller100% (3)
- Alcohol Withdrawal Care PlanDokument1 SeiteAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- Bowel ObstructionDokument48 SeitenBowel ObstructionPatrick John100% (1)
- Erectile DysfunctionDokument31 SeitenErectile Dysfunctionrahuldtc100% (1)
- Newborn Assessment NORMALDokument2 SeitenNewborn Assessment NORMALVanessaMUellerNoch keine Bewertungen
- Holistic Perspective of Physical TherapyDokument31 SeitenHolistic Perspective of Physical TherapyShimmering MoonNoch keine Bewertungen
- Antiarrhythmic Drugs 1Dokument32 SeitenAntiarrhythmic Drugs 1AliImadAlKhasakiNoch keine Bewertungen
- AMRI Hospital TariffDokument42 SeitenAMRI Hospital TariffsandeepNoch keine Bewertungen
- COPD Care PLAN PDFDokument2 SeitenCOPD Care PLAN PDFVanessaMUeller100% (1)
- Nebulizing & Suctioning TechniquesDokument23 SeitenNebulizing & Suctioning TechniquesRifky Octavio PNoch keine Bewertungen
- Comprehensive Head To Toe Assessment PDFDokument22 SeitenComprehensive Head To Toe Assessment PDFVanessaMUellerNoch keine Bewertungen
- Chughtai Lab Rate ListDokument33 SeitenChughtai Lab Rate ListHassan Gill67% (9)
- Bronchoscopy: Dr. Ravi Gadani MS, FmasDokument17 SeitenBronchoscopy: Dr. Ravi Gadani MS, FmasRaviNoch keine Bewertungen
- Alcohol Withdrawal Care PlanDokument1 SeiteAlcohol Withdrawal Care PlanVanessaMUellerNoch keine Bewertungen
- Physical Assessment ChartDokument1 SeitePhysical Assessment ChartVanessaMUellerNoch keine Bewertungen
- Example 1 - Focus: Nausea Related To AnestheticDokument1 SeiteExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerNoch keine Bewertungen
- ManagmentDokument1 SeiteManagmentVanessaMUellerNoch keine Bewertungen
- Updated Clinical SheetDokument1 SeiteUpdated Clinical SheetVanessaMUellerNoch keine Bewertungen
- Penuemonia Care PalnDokument2 SeitenPenuemonia Care PalnVanessaMUellerNoch keine Bewertungen
- Name Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXDokument1 SeiteName Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXVanessaMUellerNoch keine Bewertungen
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDokument1 SeiteFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerNoch keine Bewertungen
- Admission Database PDFDokument6 SeitenAdmission Database PDFVanessaMUellerNoch keine Bewertungen
- Diseases With Dermatologic ManifestationsDokument1 SeiteDiseases With Dermatologic ManifestationsVanessaMUellerNoch keine Bewertungen
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDokument1 SeiteFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerNoch keine Bewertungen
- AdmimDokument2 SeitenAdmimVanessaMUellerNoch keine Bewertungen
- IV PushDokument3 SeitenIV PushVanessaMUeller100% (1)
- Clinical AssessementDokument2 SeitenClinical AssessementVanessaMUellerNoch keine Bewertungen
- Example 1 - Focus: Nausea Related To AnestheticDokument1 SeiteExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerNoch keine Bewertungen
- (Chapter 3) : Cell BiologyDokument80 Seiten(Chapter 3) : Cell BiologyVanessaMUellerNoch keine Bewertungen
- Medication Guide with Side Effects and UsesDokument10 SeitenMedication Guide with Side Effects and UsesVanessaMUellerNoch keine Bewertungen
- Nurse Brain Sheet Half SizeDokument1 SeiteNurse Brain Sheet Half SizeRobyn GrogitskyNoch keine Bewertungen
- Wound Care PDFDokument100 SeitenWound Care PDFVanessaMUellerNoch keine Bewertungen
- HR Ocampo Danilo s2 E10 PDFDokument4 SeitenHR Ocampo Danilo s2 E10 PDFVanessaMUellerNoch keine Bewertungen
- Chapter 4 A1 Poster Example 2Dokument3 SeitenChapter 4 A1 Poster Example 2Krisna PamungkasNoch keine Bewertungen
- Colorectal CancerDokument23 SeitenColorectal Cancerralph_gail100% (1)
- C1963 D 01Dokument116 SeitenC1963 D 01Драган Столовић25% (4)
- Ultrasound-Guided Brachial Plexus BlockDokument7 SeitenUltrasound-Guided Brachial Plexus BlockÇağdaş BaytarNoch keine Bewertungen
- Lecture Notes General SurgeryDokument16 SeitenLecture Notes General SurgeryHamsa VeniNoch keine Bewertungen
- Coverage Midterm Examination 2021 Drug and Vice ControlDokument4 SeitenCoverage Midterm Examination 2021 Drug and Vice ControlTaga Phase 7Noch keine Bewertungen
- UNAIDS Core Epidemiology Slides enDokument11 SeitenUNAIDS Core Epidemiology Slides enTabarcea VitaliNoch keine Bewertungen
- Covid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaDokument6 SeitenCovid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaIJAR JOURNALNoch keine Bewertungen
- The Sage Encyclopedia of Abnormal and Clinical Psychology - I36172Dokument5 SeitenThe Sage Encyclopedia of Abnormal and Clinical Psychology - I36172Rol AnimeNoch keine Bewertungen
- Daftar Diagnosa Borang Dokter InternsipDokument13 SeitenDaftar Diagnosa Borang Dokter InternsipAnonymous WKPdl5rTNoch keine Bewertungen
- DM GerontikDokument15 SeitenDM GerontikPuji Affan Dwi MiriyantoNoch keine Bewertungen
- Case Presentation Hepatitis A LuluDokument28 SeitenCase Presentation Hepatitis A LuluBrenda KarinaNoch keine Bewertungen
- Reaksi Hipersensitivitas Atau Alergi: RiwayatiDokument7 SeitenReaksi Hipersensitivitas Atau Alergi: Riwayatiaulia nissaNoch keine Bewertungen
- DCMNTDokument2 SeitenDCMNTameenNoch keine Bewertungen
- Pe 1 Module 1Dokument11 SeitenPe 1 Module 1Joanna Valerie A. IboñaNoch keine Bewertungen
- Recuperare 1Dokument3 SeitenRecuperare 1Mihnea TurcuNoch keine Bewertungen
- SulpirideDokument4 SeitenSulpirideIsmail Ali SyahbanaNoch keine Bewertungen
- Dementia Conversion DisordersDokument28 SeitenDementia Conversion DisordersAYO NELSON100% (1)
- NstiDokument12 SeitenNstiKania IradatyaNoch keine Bewertungen
- Curriculum Vitae of Professor Francesco RiaDokument9 SeitenCurriculum Vitae of Professor Francesco RianoncanimussurdisNoch keine Bewertungen
- OSCE Subcutaneous Injection SkillsDokument2 SeitenOSCE Subcutaneous Injection SkillsvishnuNoch keine Bewertungen