Das könnte Ihnen auch gefallen
- Diagnostic Tests in Pediatric Pulmonology: Applications and InterpretationVon EverandDiagnostic Tests in Pediatric Pulmonology: Applications and InterpretationStephanie D. DavisNoch keine Bewertungen
- NIH Public AccessDokument13 SeitenNIH Public AccessEndah susantiNoch keine Bewertungen
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareVon EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNoch keine Bewertungen
- Evaluation of The Children With Acute Acetaminophen Overdose and Intravenous N-Acetylcysteine TreatmentDokument5 SeitenEvaluation of The Children With Acute Acetaminophen Overdose and Intravenous N-Acetylcysteine Treatmentdiajeng ayuNoch keine Bewertungen
- Nejmoa1911998 PDFDokument11 SeitenNejmoa1911998 PDFStella NoviaNoch keine Bewertungen
- S177 Full PDFDokument4 SeitenS177 Full PDFCalvin AffendyNoch keine Bewertungen
- Acetaminophen and Ibuprofen in The Treatment of Pediatric Fever A Narrative ReviewDokument14 SeitenAcetaminophen and Ibuprofen in The Treatment of Pediatric Fever A Narrative ReviewI Made AryanaNoch keine Bewertungen
- Jamapediatrics Wang 2021 Oi 200094 1616606175.10588Dokument10 SeitenJamapediatrics Wang 2021 Oi 200094 1616606175.10588Fabiola Vania FeliciaNoch keine Bewertungen
- Efikasi Ibuprofen & PCT Meta AnalisisDokument18 SeitenEfikasi Ibuprofen & PCT Meta AnalisisdeviaelfkNoch keine Bewertungen
- The Safety of Acetaminophen and Ibuprofen Among Children Younger Than Two Years OldDokument7 SeitenThe Safety of Acetaminophen and Ibuprofen Among Children Younger Than Two Years OldsastiraNoch keine Bewertungen
- Contoh UTBK SoshumDokument6 SeitenContoh UTBK SoshumsalshabilaNoch keine Bewertungen
- Epinephrine and Dexamethasone in Children With BronchiolitisDokument11 SeitenEpinephrine and Dexamethasone in Children With BronchiolitisAdelina Wahyuni LubisNoch keine Bewertungen
- Rosenbloom 2013Dokument4 SeitenRosenbloom 2013Imam SabarudinNoch keine Bewertungen
- Sample Critics RTCDokument12 SeitenSample Critics RTCGada NagariNoch keine Bewertungen
- Cáncer y Paracetamol ArticuloDokument10 SeitenCáncer y Paracetamol ArticuloChrystian Saavedra santosNoch keine Bewertungen
- Efficacy of Minor Analgesics in Primary Dysmenorrhoea: Systematic ReviewDokument10 SeitenEfficacy of Minor Analgesics in Primary Dysmenorrhoea: Systematic Reviewadi saputraNoch keine Bewertungen
- 2 PDFDokument8 Seiten2 PDFsastiraNoch keine Bewertungen
- Ene 15103Dokument8 SeitenEne 15103Natalia E PenagosNoch keine Bewertungen
- 2010 Early CPAP Vs Surfactant in EPTI NEJMDokument10 Seiten2010 Early CPAP Vs Surfactant in EPTI NEJMFiorella VilcaNoch keine Bewertungen
- Thorax 2003 White 317 21Dokument6 SeitenThorax 2003 White 317 21AlejandroNoch keine Bewertungen
- JOurnal PatricioDokument2 SeitenJOurnal PatricioMarjorie ChingNoch keine Bewertungen
- Cpap Vs SurfactanteDokument10 SeitenCpap Vs SurfactanteAngelicia Varela MuñozNoch keine Bewertungen
- Jurnal AsthmaDokument11 SeitenJurnal AsthmaNadira Juanti PratiwiNoch keine Bewertungen
- Badger MejmDokument11 SeitenBadger Mejmalfred1294Noch keine Bewertungen
- Pediatric PharmacotherapyDokument4 SeitenPediatric PharmacotherapyRiriNoch keine Bewertungen
- 2006-Long-Term Use of Oxcarbazepine Oral Suspension in Childhood Epilepsy - Open-Label Study PDFDokument6 Seiten2006-Long-Term Use of Oxcarbazepine Oral Suspension in Childhood Epilepsy - Open-Label Study PDFAnonymous bEwTSXJ1gNoch keine Bewertungen
- Preventing Preeclampsia With Aspirin Does Dose or Timing Matter - 2017 - American Journal of Obstetrics and Gynecology PDFDokument3 SeitenPreventing Preeclampsia With Aspirin Does Dose or Timing Matter - 2017 - American Journal of Obstetrics and Gynecology PDFfujimeisterNoch keine Bewertungen
- Asma 2Dokument7 SeitenAsma 2alexvamaNoch keine Bewertungen
- Safety of Adding Salmeterol To Fluticasone Propionate in Children With AsthmaDokument19 SeitenSafety of Adding Salmeterol To Fluticasone Propionate in Children With AsthmaQonita Aizati QomaruddinNoch keine Bewertungen
- Peds 2013-2404 FullDokument10 SeitenPeds 2013-2404 FullAditya Pratama SaaninNoch keine Bewertungen
- Jurnal Anak RirinDokument10 SeitenJurnal Anak RirinDexter BluesNoch keine Bewertungen
- Controlled Trial Lansoprazole For Children With Poorly Controlled Asthma: A RandomizedDokument4 SeitenControlled Trial Lansoprazole For Children With Poorly Controlled Asthma: A RandomizedJames HollandNoch keine Bewertungen
- Artikel TherapyDokument6 SeitenArtikel TherapyKyra ModestyNoch keine Bewertungen
- JURNAL READINGnejmoa1007174Dokument11 SeitenJURNAL READINGnejmoa1007174Sukma WinahyuNoch keine Bewertungen
- Article 10Dokument7 SeitenArticle 10vzwsvt7hgkNoch keine Bewertungen
- 67 FullDokument8 Seiten67 FulljessicacookNoch keine Bewertungen
- Prospectivo - Grunwell2017Dokument8 SeitenProspectivo - Grunwell2017MecheVSNoch keine Bewertungen
- Pi Is 0091674918312788Dokument31 SeitenPi Is 0091674918312788muhammad_ariefNoch keine Bewertungen
- Trial of Amitriptyline, Topiramate, and Placebo For Pediatric MigraineDokument10 SeitenTrial of Amitriptyline, Topiramate, and Placebo For Pediatric Migraineaditya7Noch keine Bewertungen
- Pediatrics 2011 Mahr S129 30Dokument4 SeitenPediatrics 2011 Mahr S129 30Erlangga Perwira NegaraNoch keine Bewertungen
- Kim 2016Dokument9 SeitenKim 2016Victoria NatashaNoch keine Bewertungen
- Wait-and-See Prescription For The Treatment of Acute Otitis MediaDokument7 SeitenWait-and-See Prescription For The Treatment of Acute Otitis MediaatikahanifahNoch keine Bewertungen
- Risk of Asthma Exacerbation Associated With.32Dokument8 SeitenRisk of Asthma Exacerbation Associated With.32xiongmao2389Noch keine Bewertungen
- Cummings 2015Dokument11 SeitenCummings 2015MaluNoch keine Bewertungen
- Fernandez, John Michael BSN403 Group 10: I. Clinical QuestionDokument5 SeitenFernandez, John Michael BSN403 Group 10: I. Clinical QuestionJohn Michael FernandezNoch keine Bewertungen
- ASMA2006Dokument10 SeitenASMA2006OscarDavidGordilloGonzalezNoch keine Bewertungen
- Nejmoa 1814917Dokument11 SeitenNejmoa 1814917yasserNoch keine Bewertungen
- Increase 1.Dokument10 SeitenIncrease 1.Maria Jose Contreras SilvaNoch keine Bewertungen
- Inhaled Corticosteroids and Respiratory Infections in Children With Asthma: A Meta-AnalysisDokument17 SeitenInhaled Corticosteroids and Respiratory Infections in Children With Asthma: A Meta-AnalysisHanida Rahmah TaminNoch keine Bewertungen
- Uso de Premedicacion Intubacion 2018 CartaDokument2 SeitenUso de Premedicacion Intubacion 2018 CartaJorge CastroNoch keine Bewertungen
- Pediatric Pharmacology and TherapeuticsDokument6 SeitenPediatric Pharmacology and TherapeuticsRatna SriwahyuniNoch keine Bewertungen
- The PAIN Study: Paracetamol, Aspirin and Ibuprofen New Tolerability StudyDokument11 SeitenThe PAIN Study: Paracetamol, Aspirin and Ibuprofen New Tolerability StudySattar KianiNoch keine Bewertungen
- Peds 2020-0586Dokument16 SeitenPeds 2020-0586Emilio Emmanué Escobar CruzNoch keine Bewertungen
- AR101 Oral Immunotherapy For Peanut Allergy: Original ArticleDokument11 SeitenAR101 Oral Immunotherapy For Peanut Allergy: Original ArticleWXXI NewsNoch keine Bewertungen
- New England Journal Medicine: The ofDokument11 SeitenNew England Journal Medicine: The ofprabuNoch keine Bewertungen
- A RCT of Oral Propranolol in Infantile HemangiomaDokument12 SeitenA RCT of Oral Propranolol in Infantile HemangiomaIndahNovikaNoch keine Bewertungen
- Dupilumab AsthmaDokument11 SeitenDupilumab AsthmaMr. LNoch keine Bewertungen
- S177 FullDokument4 SeitenS177 FullCalvin AffendyNoch keine Bewertungen
- Benson Multicentre 1986Dokument4 SeitenBenson Multicentre 1986Dian NovitasariNoch keine Bewertungen
- Youthful PopulationsDokument18 SeitenYouthful PopulationsJamesy66Noch keine Bewertungen
- Prgm-Sminr Faculties Identified Through FIP NIRCDokument9 SeitenPrgm-Sminr Faculties Identified Through FIP NIRCDonor CrewNoch keine Bewertungen
- Closing Ceremony PresentationDokument79 SeitenClosing Ceremony Presentationapi-335718710Noch keine Bewertungen
- Xi'an City Sports Park Landscape Improvement ProjectDokument3 SeitenXi'an City Sports Park Landscape Improvement ProjectGirija Sankar SahuNoch keine Bewertungen
- 10 Ideas For ConversationDokument116 Seiten10 Ideas For ConversationGreenLake36100% (1)
- Roy II vs. Herbosa, G.R. No. 207946, November 22, 2016Dokument20 SeitenRoy II vs. Herbosa, G.R. No. 207946, November 22, 2016Rina OlandoNoch keine Bewertungen
- MKT305 (Module 6 Segmentation)Dokument53 SeitenMKT305 (Module 6 Segmentation)Ngọc AnhhNoch keine Bewertungen
- Preparatory Surface Cleaning of Architectural Sandstone: Standard Practice ForDokument2 SeitenPreparatory Surface Cleaning of Architectural Sandstone: Standard Practice Fors.swamyNoch keine Bewertungen
- 20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánDokument131 Seiten20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánThanh NganNoch keine Bewertungen
- Case Analysis OF Rajinder Singh V. State of PunjabDokument12 SeitenCase Analysis OF Rajinder Singh V. State of PunjabP TejeswariNoch keine Bewertungen
- Treason Cases Digested (Crim Law 2)Dokument5 SeitenTreason Cases Digested (Crim Law 2)Jacob Castro100% (2)
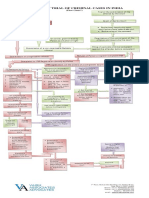
- Process of Trial of Criminal Cases in India (Flow Chart)Dokument1 SeiteProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Creative WritingDokument13 SeitenCreative WritingBeberly Kim AmaroNoch keine Bewertungen
- Full Download Test Bank For Ethics Theory and Contemporary Issues 9th Edition Mackinnon PDF Full ChapterDokument36 SeitenFull Download Test Bank For Ethics Theory and Contemporary Issues 9th Edition Mackinnon PDF Full Chapterpapismlepal.b8x1100% (16)
- Practical No 4Dokument5 SeitenPractical No 4Mahin SarkarNoch keine Bewertungen
- Personal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulDokument6 SeitenPersonal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulKanchanNoch keine Bewertungen
- Ingles V Eje 1 Week 2Dokument5 SeitenIngles V Eje 1 Week 2Cristhian Javier Torres PenaNoch keine Bewertungen
- Comics Trip MasterpiecesDokument16 SeitenComics Trip MasterpiecesDaniel Constantine100% (2)
- 2020 DepEd English Proficiency Test (EPT) Reviewer - TeacherPHDokument205 Seiten2020 DepEd English Proficiency Test (EPT) Reviewer - TeacherPHAlron GAmboa100% (1)
- National Highways Authority of IndiaDokument3 SeitenNational Highways Authority of IndiaRohitNoch keine Bewertungen
- Chem HazardsDokument17 SeitenChem HazardsMJ NuarinNoch keine Bewertungen
- Ermita Malate Hotel Motel Operators V City Mayor DigestDokument1 SeiteErmita Malate Hotel Motel Operators V City Mayor Digestpnp bantay100% (2)
- SDS Jojoba Wax Beads 2860Dokument7 SeitenSDS Jojoba Wax Beads 2860swerNoch keine Bewertungen
- George Herbert Scherff Walker Bush: Agentur of The New World OrderDokument36 SeitenGeorge Herbert Scherff Walker Bush: Agentur of The New World Orderextemporaneous100% (3)
- Quantum PauseDokument5 SeitenQuantum Pausesoulsearch67641100% (2)
- Mushaf Qiraat Asim - (Syukbah)Dokument604 SeitenMushaf Qiraat Asim - (Syukbah)amnrs88100% (1)
- Grid / Hippodamian Model: Hippodamus of MiletusDokument34 SeitenGrid / Hippodamian Model: Hippodamus of MiletusVriti SachdevaNoch keine Bewertungen
- Cloud Native 5G Core Samsung 5G Core Volume 2Dokument16 SeitenCloud Native 5G Core Samsung 5G Core Volume 2ALEXANDRE JOSE FIGUEIREDO LOUREIRO100% (1)
- CJ1W-PRT21 PROFIBUS-DP Slave Unit: Operation ManualDokument100 SeitenCJ1W-PRT21 PROFIBUS-DP Slave Unit: Operation ManualSergio Eu CaNoch keine Bewertungen
- Brief CVDokument6 SeitenBrief CVDocument ReservedNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (35)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeVon EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (44)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingVon EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingBewertung: 1 von 5 Sternen1/5 (2)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Von EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Bewertung: 5 von 5 Sternen5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsVon EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNoch keine Bewertungen
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)