Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Oil Gas Midstream BFC 2018Dokument22 SeitenOil Gas Midstream BFC 2018zakaria aouamNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Geography Paper 4 Flashcards-2Dokument16 SeitenGeography Paper 4 Flashcards-2faryal khanNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Ken Black QA All Odd No Chapter SolutionDokument919 SeitenKen Black QA All Odd No Chapter SolutionRushabh Vora83% (6)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- CompositesWorld July 2021Dokument52 SeitenCompositesWorld July 2021Shin JoonHoNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Facility Layout Case StudyDokument8 SeitenFacility Layout Case StudyHitesh SinglaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- TQM and Supply Chian Management Similalities and DifferencesDokument13 SeitenTQM and Supply Chian Management Similalities and DifferencesrnaganirmitaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Behavior Prediction Through Handwriting Analysis: Parmeet Kaur Grewal, Deepak PrasharDokument4 SeitenBehavior Prediction Through Handwriting Analysis: Parmeet Kaur Grewal, Deepak PrasharqwerNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Aml Programs Module 4 Quiz AnswersDokument8 SeitenAml Programs Module 4 Quiz AnswersAmir SiddiquiNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Visvesvaraya Technological University, BelagaviDokument67 SeitenVisvesvaraya Technological University, BelagaviAKSHAYKUMAR JAMADARNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- BUS 5111 - Financial Management-Portfolio Activity Unit 1Dokument4 SeitenBUS 5111 - Financial Management-Portfolio Activity Unit 1LaVida LocaNoch keine Bewertungen
- KINGFISHER-BEER-Vasantha Naik .LDokument85 SeitenKINGFISHER-BEER-Vasantha Naik .Lushadgs100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Resource H Approaching The Literature Review PowerpointDokument16 SeitenResource H Approaching The Literature Review PowerpointAnonymous XTL7o0tGo9Noch keine Bewertungen
- The Teochew Chinese of ThailandDokument7 SeitenThe Teochew Chinese of ThailandbijsshrjournalNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The New Empirical Formula Based On Dynamic Probing Test Results in Fine Cohesive SoilsDokument10 SeitenThe New Empirical Formula Based On Dynamic Probing Test Results in Fine Cohesive SoilsabualamalNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Projective Technique: Business Research MethodsDokument25 SeitenProjective Technique: Business Research MethodsSandhya DubeyNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Chapter: 1 Introduction To Research: Instructor: Dr. Vikrant ShagaDokument22 SeitenChapter: 1 Introduction To Research: Instructor: Dr. Vikrant Shagatrisit mulatNoch keine Bewertungen
- Fractions Final ProjectDokument10 SeitenFractions Final Projectapi-291564354Noch keine Bewertungen
- FloridathesisDokument28 SeitenFloridathesisrichardbarcinilla02Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Child-Friendly SchoolDokument21 SeitenChild-Friendly SchoolJovi Buizon Lopez100% (21)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Top Performing K To 3 Pupils' Unfamiliarity With The Ibanag Words Used in Modules As Described by The TeachersDokument12 SeitenTop Performing K To 3 Pupils' Unfamiliarity With The Ibanag Words Used in Modules As Described by The TeachersPsychology and Education: A Multidisciplinary JournalNoch keine Bewertungen
- Analysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationDokument4 SeitenAnalysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationMahavir GemavatNoch keine Bewertungen
- ZomatoDokument7 SeitenZomatoRenieNoch keine Bewertungen
- Difference Between Thesis and Dissertation UkDokument7 SeitenDifference Between Thesis and Dissertation Ukaflpbevnrabaqk100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Forrester - The Current State of Marketing Measurement and OptimizationDokument17 SeitenForrester - The Current State of Marketing Measurement and OptimizationLadyboy Sissy ChristianeNoch keine Bewertungen
- RM AssignmentDokument2 SeitenRM Assignmentanugraha vasanNoch keine Bewertungen
- Placebo-Controlled Trial of Amantadine For Severe Traumatic Brain Injury - NEJMDokument2 SeitenPlacebo-Controlled Trial of Amantadine For Severe Traumatic Brain Injury - NEJMJamesHowsonNoch keine Bewertungen
- Diabetes Essay ConclusionDokument6 SeitenDiabetes Essay Conclusiond3h7qfpr100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
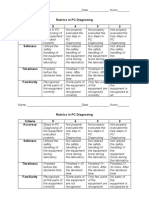
- Rubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - ScoreDokument2 SeitenRubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - Scorejhun ecleoNoch keine Bewertungen
- Writing - Free Writing Short NarrativeDokument11 SeitenWriting - Free Writing Short NarrativeSaravana SelvakumarNoch keine Bewertungen
- OrganizingDokument46 SeitenOrganizingViswajeet BiswalNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)