Das könnte Ihnen auch gefallen
- Acetylcholine Stimulates Muscle Contraction in Guinea Pig Ileum and Atropine Diminishes The Extent of ContractionDokument2 SeitenAcetylcholine Stimulates Muscle Contraction in Guinea Pig Ileum and Atropine Diminishes The Extent of Contractionleh.mo931580% (5)
- STEPPS For NEA-BPD Call-In Series June 8 2014 - Part 1Dokument24 SeitenSTEPPS For NEA-BPD Call-In Series June 8 2014 - Part 1Aaser Aasde100% (2)
- All HAAD Forms 2015-2019Dokument37 SeitenAll HAAD Forms 2015-2019SherinNoch keine Bewertungen
- Cholinergics and AnticholinergicsDokument5 SeitenCholinergics and AnticholinergicscatislandbigredNoch keine Bewertungen
- Obat Asma: Irme Adhitya 21804101051 Pembimbing: Andri Tilaqza, S.Farm, M.Farm, AptDokument85 SeitenObat Asma: Irme Adhitya 21804101051 Pembimbing: Andri Tilaqza, S.Farm, M.Farm, AptIrme AdhityaNoch keine Bewertungen
- Pharmacokinetics and Comparative Bioavailability of Allopurinol Formulations in Healthy SubjectsDokument5 SeitenPharmacokinetics and Comparative Bioavailability of Allopurinol Formulations in Healthy SubjectsFajar NovendraNoch keine Bewertungen
- Chapter 8. Cholinoceptor-Blocking DrugsDokument4 SeitenChapter 8. Cholinoceptor-Blocking Drugsridoy2146Noch keine Bewertungen
- Ijac2021 5558651Dokument12 SeitenIjac2021 5558651Darian HerascuNoch keine Bewertungen
- Effect of Single and Repeated Doses of Ketoconazole On The Pharmacokinetics of RoflumilastDokument12 SeitenEffect of Single and Repeated Doses of Ketoconazole On The Pharmacokinetics of RoflumilastLuciana OliveiraNoch keine Bewertungen
- JPBAS 1 (2) 3chitralekha SainiDokument7 SeitenJPBAS 1 (2) 3chitralekha SainiHarish KakraniNoch keine Bewertungen
- Adrenergic AgentsDokument7 SeitenAdrenergic AgentsMuhamed ArsalanNoch keine Bewertungen
- Petroianu 2005Dokument5 SeitenPetroianu 2005Bilel ChefiratNoch keine Bewertungen
- Ligustrazine Phosphate Ethosomes For Treatment of Alzheimer's Disease, in Vitro and in Animal Model StudiesDokument8 SeitenLigustrazine Phosphate Ethosomes For Treatment of Alzheimer's Disease, in Vitro and in Animal Model Studiesebooks list1Noch keine Bewertungen
- Strattera LBLDokument21 SeitenStrattera LBLDermot BrennanNoch keine Bewertungen
- Tropane: Hyoscyamine and Hyoscine. Also, We Can Find Scopolamine and CalysteginesDokument6 SeitenTropane: Hyoscyamine and Hyoscine. Also, We Can Find Scopolamine and Calysteginesmumen abusadahNoch keine Bewertungen
- Jurnal 2Dokument11 SeitenJurnal 2Isnaini AnnurNoch keine Bewertungen
- Mefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Dokument20 SeitenMefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Riska AuliahNoch keine Bewertungen
- Anti Asthamatic DrugsDokument28 SeitenAnti Asthamatic DrugsGOPALNoch keine Bewertungen
- The Influence of CYP2D6 Phenotype On The Pharmacokinetic Profile of Atomoxetine in Caucasian Healthy SubjectsDokument8 SeitenThe Influence of CYP2D6 Phenotype On The Pharmacokinetic Profile of Atomoxetine in Caucasian Healthy SubjectsAlina RotariNoch keine Bewertungen
- CarbamateDokument7 SeitenCarbamateJulianHCardenasNoch keine Bewertungen
- Analytical Methods OriDokument18 SeitenAnalytical Methods OriHarsh KoshtiNoch keine Bewertungen
- B Pharm Sem 1Dokument28 SeitenB Pharm Sem 1prajwalshende916Noch keine Bewertungen
- Captopril: Determination in Blood and Pharmacokinetics After Single Oral DoseDokument6 SeitenCaptopril: Determination in Blood and Pharmacokinetics After Single Oral DoseKhintan Risky FadhilaNoch keine Bewertungen
- Degradation PramipexoleDokument9 SeitenDegradation Pramipexoleclaudiamaniac7Noch keine Bewertungen
- The Evaluation of Antioxidant Potential PDFDokument10 SeitenThe Evaluation of Antioxidant Potential PDFEgaSulsitiyoNingrumNoch keine Bewertungen
- S 002 LBLDokument35 SeitenS 002 LBLRDZENNoch keine Bewertungen
- Drug Metabolism - Chapter 8Dokument44 SeitenDrug Metabolism - Chapter 8Shaun李好Noch keine Bewertungen
- Validated Spectrophotometric Method For The Determination of Chloramphenicol in Pure and in Its Dosage FormDokument6 SeitenValidated Spectrophotometric Method For The Determination of Chloramphenicol in Pure and in Its Dosage FormNin TiyasNoch keine Bewertungen
- Padmaja2017 PDFDokument10 SeitenPadmaja2017 PDFmanoj bhattaraiNoch keine Bewertungen
- 01 TKD Tiu CPNSDokument5 Seiten01 TKD Tiu CPNSRaisa NurhijriyahNoch keine Bewertungen
- Chlorpromazine: Pharmacology Indications Contraindications Precautions Adverse Effects Overdose Dosage ResearchDokument36 SeitenChlorpromazine: Pharmacology Indications Contraindications Precautions Adverse Effects Overdose Dosage Researchnwaon4realNoch keine Bewertungen
- SY - Medichem I - ParasympathomimeticsDokument96 SeitenSY - Medichem I - ParasympathomimeticsKevalNoch keine Bewertungen
- The Human Pharmacology of Fluticasone PropionateDokument5 SeitenThe Human Pharmacology of Fluticasone PropionatePavel MilovNoch keine Bewertungen
- 2010 Determination of Aspirin Tablets From Different Industrial Drug Companies Available in Iraqi Pharmaceutical MarketDokument14 Seiten2010 Determination of Aspirin Tablets From Different Industrial Drug Companies Available in Iraqi Pharmaceutical MarketCristian David Villa DiazNoch keine Bewertungen
- Pharmacology Viva Manual Prefinal PDFDokument112 SeitenPharmacology Viva Manual Prefinal PDF9821699080100% (1)
- Effect of Omeprazole On Oral and Intravenous RS-Methadone Pharmacokinetics and Pharmacodynamics in The RatDokument12 SeitenEffect of Omeprazole On Oral and Intravenous RS-Methadone Pharmacokinetics and Pharmacodynamics in The Ratdian oktavianiNoch keine Bewertungen
- AbstractDokument11 SeitenAbstractKeshav HiraveNoch keine Bewertungen
- AmphetamineDokument15 SeitenAmphetamineIoanaTănaseNoch keine Bewertungen
- Cholinoceptor AntagonistDokument21 SeitenCholinoceptor Antagonistraafat mohammedNoch keine Bewertungen
- Final Draft EsomeprazoleDokument4 SeitenFinal Draft EsomeprazoleHassan Raza GilalNoch keine Bewertungen
- A Review of The Clinical Pharmacokinetics of MeloxicamDokument4 SeitenA Review of The Clinical Pharmacokinetics of MeloxicamkwadwobrosNoch keine Bewertungen
- Enzyme Inhibition Studies of AntipyrineDokument10 SeitenEnzyme Inhibition Studies of Antipyrineشمس صبيح عبد الرحيمNoch keine Bewertungen
- Farmako PDFDokument16 SeitenFarmako PDFIsney HanindyaNoch keine Bewertungen
- TramadolDokument6 SeitenTramadolMirabilis MinoNoch keine Bewertungen
- DR +Abhishek+SoniDokument7 SeitenDR +Abhishek+SoniSivesh VersionNoch keine Bewertungen
- Timolol 2Dokument8 SeitenTimolol 2EMANUEL CAMILO MARTINEZ VILLAMIZARNoch keine Bewertungen
- Amoxicillin 1Dokument8 SeitenAmoxicillin 1Prince AliNoch keine Bewertungen
- LojDokument11 SeitenLojDrkrishnasarma pathyNoch keine Bewertungen
- Parasympathomimetics and ParasympatholyticsDokument16 SeitenParasympathomimetics and ParasympatholyticsSalona Roy100% (4)
- Phytotherapy Research Volume 24 Issue 3 2010 (Doi 10.1002/ptr.2982) Hyung-In Moon Ill-Min Chung Su-Hyun SEO Eun-Young Kang - Protective Effects of 3 - Deoxy-4-O-methylepiDokument3 SeitenPhytotherapy Research Volume 24 Issue 3 2010 (Doi 10.1002/ptr.2982) Hyung-In Moon Ill-Min Chung Su-Hyun SEO Eun-Young Kang - Protective Effects of 3 - Deoxy-4-O-methylepiFaradita NindyasariNoch keine Bewertungen
- Disposition of Acamprosate in The Rat: Influence of ProbenecidDokument9 SeitenDisposition of Acamprosate in The Rat: Influence of ProbenecidCLPHtheoryNoch keine Bewertungen
- 2016 - Inflammopharmacology - Sokmen Et Al - The Antioxidant Activity of Some CurcuminoidsDokument6 Seiten2016 - Inflammopharmacology - Sokmen Et Al - The Antioxidant Activity of Some CurcuminoidsNadia ErlinaNoch keine Bewertungen
- Pharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyDokument9 SeitenPharmacokinetic Interaction Between Fluoxetine and Omeprazole in Healthy Male Volunteers: A Prospective Pilot StudyCurcubeuAuroraNoch keine Bewertungen
- Midterms Topic 5Dokument21 SeitenMidterms Topic 5Lara GatbontonNoch keine Bewertungen
- Investigation of Antioxidant Activity and Total Phenolic Content of Various Fractions of Aerial Parts of Pimpinella Barbata (DC.) BoissDokument5 SeitenInvestigation of Antioxidant Activity and Total Phenolic Content of Various Fractions of Aerial Parts of Pimpinella Barbata (DC.) BoissBrenda D'AcunhaNoch keine Bewertungen
- Development and Evaluation of Buccoadhesive Propranolol Hudrochloride Tablet Formulations Effect of FillersDokument7 SeitenDevelopment and Evaluation of Buccoadhesive Propranolol Hudrochloride Tablet Formulations Effect of FillersCesar Rodolfo Angulo DelgadoNoch keine Bewertungen
- Caffeine Enhances The Antidepressant-Like Activity of Common Antidepressant Drugs in The Forced Swim Test in MiceDokument11 SeitenCaffeine Enhances The Antidepressant-Like Activity of Common Antidepressant Drugs in The Forced Swim Test in MiceMutiara ApriliansyahNoch keine Bewertungen
- Activity 11 MetabolismDokument6 SeitenActivity 11 MetabolismdavenNoch keine Bewertungen
- Phama Exam.Dokument14 SeitenPhama Exam.muwonge benonNoch keine Bewertungen
- Pharmacokinetics of AdderallDokument29 SeitenPharmacokinetics of AdderallhsxvskgtrhNoch keine Bewertungen
- Kalambe Sai FinalDokument13 SeitenKalambe Sai FinalKeshav HiraveNoch keine Bewertungen
- Advances in Dopamine Research: Proceeding of a Satellite Symposium to the 8th International Congress of Pharmacology, Okayama, Japan, July 1981Von EverandAdvances in Dopamine Research: Proceeding of a Satellite Symposium to the 8th International Congress of Pharmacology, Okayama, Japan, July 1981M. KohsakaNoch keine Bewertungen
- Medicinal Chemistry of Drugs Affecting the Nervous SystemVon EverandMedicinal Chemistry of Drugs Affecting the Nervous SystemNoch keine Bewertungen
- Drug Use and Abuse in Sport Ver CocainaDokument37 SeitenDrug Use and Abuse in Sport Ver CocainaAaser AasdeNoch keine Bewertungen
- Tribunal Arbitral Du Sport Court of Arbitration For SportDokument19 SeitenTribunal Arbitral Du Sport Court of Arbitration For SportAaser AasdeNoch keine Bewertungen
- Schizophrenia Research: Gordon L.F. Cheng, Joey C.Y. Tang, Frendi W.S. Li, Esther Y.Y. Lau, Tatia M.C. LeeDokument6 SeitenSchizophrenia Research: Gordon L.F. Cheng, Joey C.Y. Tang, Frendi W.S. Li, Esther Y.Y. Lau, Tatia M.C. LeeAaser AasdeNoch keine Bewertungen
- Appi Ajp 2007 07071079Dokument11 SeitenAppi Ajp 2007 07071079Aaser AasdeNoch keine Bewertungen
- Drug and Alcohol DependenceDokument8 SeitenDrug and Alcohol DependenceAaser AasdeNoch keine Bewertungen
- Clinical Pharmacology Book 2018 1Dokument304 SeitenClinical Pharmacology Book 2018 1Salman khanNoch keine Bewertungen
- Renner 2005Dokument11 SeitenRenner 2005Aaser AasdeNoch keine Bewertungen
- CH 15Dokument26 SeitenCH 15Mohd Khairidzman BoeranNoch keine Bewertungen
- Parasympathomimetic DrugsDokument29 SeitenParasympathomimetic DrugsChAwais100% (1)
- Veterinary Neuropharmacology VPT 321 Lecture Notes TANUVASDokument101 SeitenVeterinary Neuropharmacology VPT 321 Lecture Notes TANUVASSunil89% (18)
- Keizer GammaDokument8 SeitenKeizer GammaBrunoNoch keine Bewertungen
- ANS - Toxic Syndromes PDFDokument74 SeitenANS - Toxic Syndromes PDFARNoch keine Bewertungen
- Effects of Temperature, Stretch, and Various Drug Treatments On The Cardiac Muscle Activity of Rana PipiensDokument15 SeitenEffects of Temperature, Stretch, and Various Drug Treatments On The Cardiac Muscle Activity of Rana PipiensAbir Hasan ShuvoNoch keine Bewertungen
- CNS Autonomic Drugs - Lecture 6Dokument35 SeitenCNS Autonomic Drugs - Lecture 6Abdullah Al-TuraifiNoch keine Bewertungen
- Human Physiology From Cells To Systems 9th Edition Sherwood Test Bank DownloadDokument24 SeitenHuman Physiology From Cells To Systems 9th Edition Sherwood Test Bank DownloadVeronica Mayhew100% (20)
- Autonomic and Systemic Pharmacology DR DahalDokument119 SeitenAutonomic and Systemic Pharmacology DR Dahalअविनाश भाल्टरNoch keine Bewertungen
- Submitted To: Assignment OnDokument35 SeitenSubmitted To: Assignment OnShahedul islamNoch keine Bewertungen
- 7-Action Drugs On BP in Intact RabbitDokument16 Seiten7-Action Drugs On BP in Intact Rabbitxq qxNoch keine Bewertungen
- UNIT6.Autonomic PharmacologyDokument66 SeitenUNIT6.Autonomic PharmacologyKaye OmoNoch keine Bewertungen
- Criselle Angeli C. Barcenas, MD, DPBA, FPSA, MmhaDokument42 SeitenCriselle Angeli C. Barcenas, MD, DPBA, FPSA, MmhachayChay gapolNoch keine Bewertungen
- Severe Asthma: Definition, Diagnosis and TreatmentDokument9 SeitenSevere Asthma: Definition, Diagnosis and TreatmentHalim Muhammad SatriaNoch keine Bewertungen
- Orgmed-1 2019Dokument165 SeitenOrgmed-1 2019Joslin Roz GalileaNoch keine Bewertungen
- Cholinergic Anticholinergic DrugsDokument60 SeitenCholinergic Anticholinergic DrugsMD. RASEL MAHMUD MIMNoch keine Bewertungen
- All DrugsDokument482 SeitenAll DrugsJessica IbañezNoch keine Bewertungen
- Organophosphate and Carbamate PoisoningDokument9 SeitenOrganophosphate and Carbamate PoisoningFabian ClavijoNoch keine Bewertungen
- Bioisosterism A Rational Approach in Drug DesignDokument30 SeitenBioisosterism A Rational Approach in Drug DesignFrancy FeltNoch keine Bewertungen
- Materi KolinergikDokument62 SeitenMateri KolinergikWira KrisnaNoch keine Bewertungen
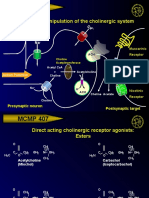
- MCMP 407: Pharmacologic Manipulation of The Cholinergic SystemDokument13 SeitenMCMP 407: Pharmacologic Manipulation of The Cholinergic System16_dev5038Noch keine Bewertungen
- Tutorial On ANS PharmacologyDokument23 SeitenTutorial On ANS PharmacologyRomaine-Ricardo FrancisNoch keine Bewertungen
- ANS, CNS KeyDokument8 SeitenANS, CNS KeyUrugonda VenumadhavNoch keine Bewertungen
- Ans Drugs Pharmacology.Dokument81 SeitenAns Drugs Pharmacology.SAMUEL - NGUNJIRINoch keine Bewertungen
- Cholinolytic DrugsDokument15 SeitenCholinolytic DrugsGeorge Kinuthia Maina100% (1)