Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Chapter 017Dokument40 SeitenChapter 017api-263755297100% (6)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Cervical Cancer BMJDokument4 SeitenCervical Cancer BMJMaria Camila Ortiz UsugaNoch keine Bewertungen
- S1578219013001431 S300 enDokument10 SeitenS1578219013001431 S300 enNurul FajrinaNoch keine Bewertungen
- Worobec2009 PDFDokument20 SeitenWorobec2009 PDFCalvin AffendyNoch keine Bewertungen
- Vir Mond 2015Dokument11 SeitenVir Mond 2015Calvin AffendyNoch keine Bewertungen
- Journal Medicine: The New EnglandDokument8 SeitenJournal Medicine: The New EnglandCalvin AffendyNoch keine Bewertungen
- Clinical Aspects of LeprosyDokument12 SeitenClinical Aspects of LeprosyChendy EndriansaNoch keine Bewertungen
- Lasik 1Dokument5 SeitenLasik 1Calvin AffendyNoch keine Bewertungen
- 444 FullDokument10 Seiten444 FullCalvin AffendyNoch keine Bewertungen
- JurnalDokument4 SeitenJurnalCalvin AffendyNoch keine Bewertungen
- E20153547 Full PDFDokument12 SeitenE20153547 Full PDFCalvin AffendyNoch keine Bewertungen
- E868 Full PDFDokument10 SeitenE868 Full PDFCalvin AffendyNoch keine Bewertungen
- P013156567 PDFDokument3 SeitenP013156567 PDFCalvin AffendyNoch keine Bewertungen
- E357 FullDokument12 SeitenE357 FullCalvin AffendyNoch keine Bewertungen
- S177 Full PDFDokument4 SeitenS177 Full PDFCalvin AffendyNoch keine Bewertungen
- Am. J. Epidemiol. 2013 Zheng Selin Aje - kws279Dokument8 SeitenAm. J. Epidemiol. 2013 Zheng Selin Aje - kws279Calvin AffendyNoch keine Bewertungen
- Fracture Risk and Zoledronic Acid Therapy in Men With OsteoporosisDokument10 SeitenFracture Risk and Zoledronic Acid Therapy in Men With OsteoporosisCalvin AffendyNoch keine Bewertungen
- Three-Year Longitudinal Survey Comparing Visual Satisfaction With LASIK and Contact LensesDokument8 SeitenThree-Year Longitudinal Survey Comparing Visual Satisfaction With LASIK and Contact LensesCalvin AffendyNoch keine Bewertungen
- Change in Axial Length Pre and Post Cataract Surgery Measured With Iolmaster 2155 9570 1000544Dokument5 SeitenChange in Axial Length Pre and Post Cataract Surgery Measured With Iolmaster 2155 9570 1000544Calvin AffendyNoch keine Bewertungen
- Cataract P ExDokument4 SeitenCataract P ExCalvin AffendyNoch keine Bewertungen
- Journal Medicine: The New EnglandDokument8 SeitenJournal Medicine: The New EnglandCalvin AffendyNoch keine Bewertungen
- E868 FullDokument10 SeitenE868 FullCalvin AffendyNoch keine Bewertungen
- E1619 Full PDFDokument11 SeitenE1619 Full PDFCalvin AffendyNoch keine Bewertungen
- Am. J. Epidemiol.-2013-Zheng Selin-Aje - kws279 PDFDokument8 SeitenAm. J. Epidemiol.-2013-Zheng Selin-Aje - kws279 PDFCalvin AffendyNoch keine Bewertungen
- Intravenous Zoledronic Acid in Postmenopausal Women With Low Bone Mineral DensityDokument9 SeitenIntravenous Zoledronic Acid in Postmenopausal Women With Low Bone Mineral DensityCalvin AffendyNoch keine Bewertungen
- E1619 Full PDFDokument11 SeitenE1619 Full PDFCalvin AffendyNoch keine Bewertungen
- E1533 Full PDFDokument10 SeitenE1533 Full PDFCalvin AffendyNoch keine Bewertungen
- S177 FullDokument4 SeitenS177 FullCalvin AffendyNoch keine Bewertungen
- Iron Supplementation in Pregnancy or Infancy and Motor Development: A Randomized Controlled TrialDokument12 SeitenIron Supplementation in Pregnancy or Infancy and Motor Development: A Randomized Controlled TrialCalvin AffendyNoch keine Bewertungen
- Toxic Anterior Segment SyndromeDokument13 SeitenToxic Anterior Segment SyndromePrathibha M ChachadiNoch keine Bewertungen
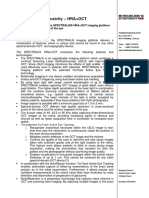
- Certificate of Exclusivity - HRA + OCT EnglishDokument4 SeitenCertificate of Exclusivity - HRA + OCT EnglishagmNoch keine Bewertungen
- AIOC 2021 Virtual. Program BookDokument508 SeitenAIOC 2021 Virtual. Program Bookmeenakshi.r.agrawalNoch keine Bewertungen
- SoalDokument8 SeitenSoalMutiara Kristiani PutriNoch keine Bewertungen
- 10th The Human Eye and The Colourful World Solved QuestionsDokument4 Seiten10th The Human Eye and The Colourful World Solved QuestionsJit AggNoch keine Bewertungen
- Project Presentation PPT FormatDokument15 SeitenProject Presentation PPT FormatJHANSI .NNoch keine Bewertungen
- Acute Bullous Keratophathy (Veterinary)Dokument3 SeitenAcute Bullous Keratophathy (Veterinary)Lorena TomoiagăNoch keine Bewertungen
- Preverbal Assessment For AmblyopiaDokument9 SeitenPreverbal Assessment For AmblyopiaLaurita RuedaNoch keine Bewertungen
- Trab Consent PDFDokument2 SeitenTrab Consent PDFRakshitha UdupiNoch keine Bewertungen
- Dwyer, AE (2016) - Oftalmología Práctica de Campo. Oftalmología Equina, 72-111.Dokument40 SeitenDwyer, AE (2016) - Oftalmología Práctica de Campo. Oftalmología Equina, 72-111.Francisco JulianNoch keine Bewertungen
- Everything About Lasik SurgeryDokument6 SeitenEverything About Lasik Surgerydrnatasha limNoch keine Bewertungen
- Abhishek PPT On TB of EyesDokument15 SeitenAbhishek PPT On TB of EyesAbhishek GuptaNoch keine Bewertungen
- The Sensitivity of The Bielschowsky Head-Tilt Test in Diagnosing Acquired Bilateral Superior Oblique ParesisDokument10 SeitenThe Sensitivity of The Bielschowsky Head-Tilt Test in Diagnosing Acquired Bilateral Superior Oblique ParesisAnonymous mvNUtwidNoch keine Bewertungen
- DOC1139 RevA-Ophthalmic Eye InstrumentCatalog PDFDokument60 SeitenDOC1139 RevA-Ophthalmic Eye InstrumentCatalog PDFMane Shubham Pradip 5-Yr IDD Civil Engg.Noch keine Bewertungen
- Adult StrabismusDokument16 SeitenAdult Strabismusmataro13Noch keine Bewertungen
- Cataract Surgery and Age Related Macular Degeneration, Recent Advances, GP and Optometist Update 2010Dokument73 SeitenCataract Surgery and Age Related Macular Degeneration, Recent Advances, GP and Optometist Update 2010Nyndia WeriNoch keine Bewertungen
- Objective Refraction Technique: Retinoscopy: Aao ReadingDokument57 SeitenObjective Refraction Technique: Retinoscopy: Aao ReadingKhairunnisaNoch keine Bewertungen
- Phacoemulsification ProcedurDokument6 SeitenPhacoemulsification Procedurnadia emildaNoch keine Bewertungen
- Prevalence and Risk Factors For Myopia Among School Children in Aba (Pdfdrive)Dokument109 SeitenPrevalence and Risk Factors For Myopia Among School Children in Aba (Pdfdrive)Esther AkwuruohaNoch keine Bewertungen
- Anatomy of The Eye PresentationDokument12 SeitenAnatomy of The Eye PresentationChalie MequanentNoch keine Bewertungen
- Analysis of Deep Learning Techniques For Prediction of Eye Diseases: A Systematic ReviewDokument34 SeitenAnalysis of Deep Learning Techniques For Prediction of Eye Diseases: A Systematic ReviewAkAnKsHa BaLiNoch keine Bewertungen
- Rotary Club of Kampala Naalya BulletinDokument4 SeitenRotary Club of Kampala Naalya BulletinDenis JjuukoNoch keine Bewertungen
- Vis AnteDokument16 SeitenVis AntejochigNoch keine Bewertungen
- Specialist: OptometryDokument16 SeitenSpecialist: OptometryChris gonzalezNoch keine Bewertungen
- 2024 Acuvue Price ListDokument2 Seiten2024 Acuvue Price Listmatt.jackson.melleNoch keine Bewertungen
- OptoPrep Part1 StudyCalendar 6-Month PDFDokument7 SeitenOptoPrep Part1 StudyCalendar 6-Month PDFmelanieNoch keine Bewertungen
- Classification: Internal UseDokument10 SeitenClassification: Internal Usejithin.rjn4055Noch keine Bewertungen
- Sonnykalangi,+38 TS +Merina+MatheosDokument5 SeitenSonnykalangi,+38 TS +Merina+MatheosNoname 149Noch keine Bewertungen
- Diagram TMGDokument20 SeitenDiagram TMGBima RizkiNoch keine Bewertungen