Das könnte Ihnen auch gefallen
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumVon EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNoch keine Bewertungen
- Cancer Immunology: Bench to Bedside Immunotherapy of CancersVon EverandCancer Immunology: Bench to Bedside Immunotherapy of CancersNoch keine Bewertungen
- Screenshot 2021-06-19 at 21.33.17Dokument11 SeitenScreenshot 2021-06-19 at 21.33.17bagus aldiNoch keine Bewertungen
- Meningitis 3Dokument12 SeitenMeningitis 3Kelly MuñozNoch keine Bewertungen
- Thwaites 2004Dokument11 SeitenThwaites 2004Navisa HaifaNoch keine Bewertungen
- Jurnal Intensified Antituberculosis Therapy in Adult With Tuberculous MeningitisDokument13 SeitenJurnal Intensified Antituberculosis Therapy in Adult With Tuberculous Meningitisnaila ghinayaNoch keine Bewertungen
- Meningitis TBDokument11 SeitenMeningitis TBErni Yessyca SimamoraNoch keine Bewertungen
- New England Journal Medicine: The ofDokument11 SeitenNew England Journal Medicine: The ofFransisca PekertiNoch keine Bewertungen
- Corticosteroids For Bacterial Meningitis in Adults in Sub-Saharan AfricaDokument10 SeitenCorticosteroids For Bacterial Meningitis in Adults in Sub-Saharan AfricaMutiara KhalishNoch keine Bewertungen
- Mortality Among Tuberculosis Patients in The Democratic Republic of CongoDokument7 SeitenMortality Among Tuberculosis Patients in The Democratic Republic of CongoGary Rios DionicioNoch keine Bewertungen
- Nejmoa1104875 TBDokument12 SeitenNejmoa1104875 TBLintang SuroyaNoch keine Bewertungen
- 6 - Iype2014Dokument7 Seiten6 - Iype2014Muhammad SyaifullahNoch keine Bewertungen
- Prevalence and Drug Resistance of Nontuberculous Mycobacteria, Northern China, 2008-2011Dokument2 SeitenPrevalence and Drug Resistance of Nontuberculous Mycobacteria, Northern China, 2008-2011Mark ReinhardtNoch keine Bewertungen
- Recurrent Glioblastoma Treated With Recombinant Poliovirus: Original ArticleDokument12 SeitenRecurrent Glioblastoma Treated With Recombinant Poliovirus: Original ArticleTrinanda ChoirunissaNoch keine Bewertungen
- Jamainternal Gopalan 2018 Oi 180003Dokument9 SeitenJamainternal Gopalan 2018 Oi 180003pentaxNoch keine Bewertungen
- Anidula VS FluconDokument11 SeitenAnidula VS FluconHarsha KuriNoch keine Bewertungen
- Necrotizing Pneumonia in Cancer Patients A.8Dokument4 SeitenNecrotizing Pneumonia in Cancer Patients A.8Manisha UppalNoch keine Bewertungen
- Paper Alumnos 3 PDFDokument10 SeitenPaper Alumnos 3 PDFVictor Martinez HagenNoch keine Bewertungen
- Transmission of Extensively Drug-Resistant Tuberculosis in South AfricaDokument11 SeitenTransmission of Extensively Drug-Resistant Tuberculosis in South AfricaDwinkha Agita PNoch keine Bewertungen
- Ahmad 2018Dokument14 SeitenAhmad 2018Cristopher OchoaNoch keine Bewertungen
- Yao 2011Dokument10 SeitenYao 2011Jemma ArakelyanNoch keine Bewertungen
- Inotozumab OzogamicinDokument14 SeitenInotozumab OzogamicinTaraNoch keine Bewertungen
- Jhe2021 6455659Dokument5 SeitenJhe2021 6455659Septi MuninggarNoch keine Bewertungen
- Early Use of TIPS in Cirrhosis and Variceal BleedingDokument10 SeitenEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liNoch keine Bewertungen
- The Clinical Outcomes and Predictive Factors For.24Dokument5 SeitenThe Clinical Outcomes and Predictive Factors For.24KeziaNoch keine Bewertungen
- Nej Mo A 1012740Dokument9 SeitenNej Mo A 1012740Mifta 'hera' Khaerati IINoch keine Bewertungen
- Long Walk TBDokument3 SeitenLong Walk TBdellanurainiNoch keine Bewertungen
- Nej Mo A 1905287Dokument12 SeitenNej Mo A 1905287Ari KurniawanNoch keine Bewertungen
- High-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisDokument10 SeitenHigh-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisSoleh SundawaNoch keine Bewertungen
- Comparison of Methicillin-Resistant Community-Acquired and Healthcare-Associated PneumoniaDokument8 SeitenComparison of Methicillin-Resistant Community-Acquired and Healthcare-Associated PneumoniaSuarniNoch keine Bewertungen
- 3 Twelve-Dose Weekly Rifapentine Plus Isoniazid For Latent TuberculosisDokument6 Seiten3 Twelve-Dose Weekly Rifapentine Plus Isoniazid For Latent TuberculosisYENIFER HOYOS MENDEZNoch keine Bewertungen
- Medi 99 E23649Dokument6 SeitenMedi 99 E23649kornelis aribowoNoch keine Bewertungen
- Langley NEJM 2014Dokument13 SeitenLangley NEJM 2014Andi MarsaliNoch keine Bewertungen
- COHORT - TB MenigealDokument11 SeitenCOHORT - TB MenigealYA MAAPNoch keine Bewertungen
- Elife 33478 v2Dokument20 SeitenElife 33478 v2Erika LlorenNoch keine Bewertungen
- Outcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudyDokument7 SeitenOutcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudylestarisurabayaNoch keine Bewertungen
- New England Journal Medicine: The ofDokument11 SeitenNew England Journal Medicine: The ofprabuNoch keine Bewertungen
- Mathur 2015Dokument7 SeitenMathur 2015Maximiliano OliveraNoch keine Bewertungen
- mdw557 2Dokument7 Seitenmdw557 2mfaddhilNoch keine Bewertungen
- Vergara C Et Al - Detection of Trypanosomacruzi by PCR in Adultswith Chronic Chagas Disease Treated With NifurtimoxDokument7 SeitenVergara C Et Al - Detection of Trypanosomacruzi by PCR in Adultswith Chronic Chagas Disease Treated With NifurtimoxjorgeNoch keine Bewertungen
- Programmes and Principles in Treatment of Multidrug-Resistant TuberculosisDokument8 SeitenProgrammes and Principles in Treatment of Multidrug-Resistant TuberculosisichacloudiacNoch keine Bewertungen
- Nej Mo A 0807381Dokument12 SeitenNej Mo A 0807381Mildred MontNoch keine Bewertungen
- AsthmaDokument10 SeitenAsthmaWidia Siti SarahNoch keine Bewertungen
- National Survey of Drug-Resistant Tuberculosis in China: June 7, 2012Dokument9 SeitenNational Survey of Drug-Resistant Tuberculosis in China: June 7, 2012galih suharnoNoch keine Bewertungen
- Microbiological Evaluation of Nosocomial Infections by Using National Nosocomial Infection Surveillance (NNIS) SystemDokument13 SeitenMicrobiological Evaluation of Nosocomial Infections by Using National Nosocomial Infection Surveillance (NNIS) SystemJanatinAzaNoch keine Bewertungen
- DexametasonDokument7 SeitenDexametasonKeniIONoch keine Bewertungen
- Nejmoa 1406281Dokument8 SeitenNejmoa 1406281zainabativeNoch keine Bewertungen
- An Exploratory Study To Assess The Knowledge Regarding Side Effects of Anti - Tubercular Drugs and Its Self-Care Management Adapted by Tuberculosis PatientsDokument8 SeitenAn Exploratory Study To Assess The Knowledge Regarding Side Effects of Anti - Tubercular Drugs and Its Self-Care Management Adapted by Tuberculosis Patientssaurabh kumar guptaNoch keine Bewertungen
- 15.benralizumab 111Dokument11 Seiten15.benralizumab 1115fqkqkcdhtNoch keine Bewertungen
- Vann Ucch I 2015Dokument10 SeitenVann Ucch I 2015gigibesiNoch keine Bewertungen
- Critical Apraisal KLPDokument11 SeitenCritical Apraisal KLPANA SRI RAHAYUNoch keine Bewertungen
- Ciw677 - TDM TB - FilsafatDokument1 SeiteCiw677 - TDM TB - FilsafatmeiyantifkusaktiNoch keine Bewertungen
- Cegielski, Levo Vs Moxi 3Dokument13 SeitenCegielski, Levo Vs Moxi 3hasan andrianNoch keine Bewertungen
- Appropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortDokument5 SeitenAppropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortSiti Annisa NurfathiaNoch keine Bewertungen
- Short-Course Intraabdominal InfectionDokument10 SeitenShort-Course Intraabdominal Infectionnicolás idárragaNoch keine Bewertungen
- Jurnal PD Convert 2Dokument14 SeitenJurnal PD Convert 2Anonymous G9gfz4Noch keine Bewertungen
- Atorvastatin Improves Sputum Conversion and Chest X-Ray Severity ScoreDokument6 SeitenAtorvastatin Improves Sputum Conversion and Chest X-Ray Severity Scorecharmainemargaret.parreno.medNoch keine Bewertungen
- M C - A P: Clinical PracticeDokument7 SeitenM C - A P: Clinical PracticeKak DhenyNoch keine Bewertungen
- Fmicb 09 01858Dokument8 SeitenFmicb 09 01858Citra CesiliaNoch keine Bewertungen
- Use of F-FDG PET To Predict Response To First-Line Tuberculostatics in HIV-Associated TuberculosisDokument6 SeitenUse of F-FDG PET To Predict Response To First-Line Tuberculostatics in HIV-Associated TuberculosisdhaniNoch keine Bewertungen
- Monkeypox Virus Infection in Humans Across 16 Countries - April-June 2022Dokument14 SeitenMonkeypox Virus Infection in Humans Across 16 Countries - April-June 2022Raphael Chalbaud Biscaia HartmannNoch keine Bewertungen
- Nejmoa 2208822Dokument12 SeitenNejmoa 2208822Gaspar PonceNoch keine Bewertungen
- New England Journal Medicine: The ofDokument10 SeitenNew England Journal Medicine: The ofMari NiculaeNoch keine Bewertungen
- New England Journal Medicine: The ofDokument10 SeitenNew England Journal Medicine: The ofMari NiculaeNoch keine Bewertungen
- Monkeypox Virus Infection in Humans Across 16 Countries - April-June 2022Dokument14 SeitenMonkeypox Virus Infection in Humans Across 16 Countries - April-June 2022Raphael Chalbaud Biscaia HartmannNoch keine Bewertungen
- Remdesivir - BeigelDokument14 SeitenRemdesivir - BeigelMaureen KoesnadiNoch keine Bewertungen
- Transcriptional Response To Interferon Beta-1a Treatment in Patients With Secondary Progressive Multiple SclerosisDokument8 SeitenTranscriptional Response To Interferon Beta-1a Treatment in Patients With Secondary Progressive Multiple SclerosisanggiNoch keine Bewertungen
- Audio Interview: Responding To Monkeypox: EditorialDokument1 SeiteAudio Interview: Responding To Monkeypox: EditorialanggiNoch keine Bewertungen
- Nej MP 2210125Dokument3 SeitenNej MP 2210125anggiNoch keine Bewertungen
- Nej MC 2200133Dokument3 SeitenNej MC 2200133anggiNoch keine Bewertungen
- Nej Me 2207596Dokument1 SeiteNej Me 2207596anggiNoch keine Bewertungen
- Nej Mic M 1701787Dokument1 SeiteNej Mic M 1701787anggiNoch keine Bewertungen
- Achieving The Triple Aim For Sexual and Gender Minorities: PerspectiveDokument4 SeitenAchieving The Triple Aim For Sexual and Gender Minorities: PerspectiveanggiNoch keine Bewertungen
- Many Authors in Business Management Research Papers Wrongly Calculate Central Tendency Just Like Wang Et Al. (2019) - This Leads To A Disaster.Dokument6 SeitenMany Authors in Business Management Research Papers Wrongly Calculate Central Tendency Just Like Wang Et Al. (2019) - This Leads To A Disaster.Scholarly CriticismNoch keine Bewertungen
- Acta Orthopaedica Et Traumatologica Turcica: H. Utkan Ayd In, Omer Berk OzDokument3 SeitenActa Orthopaedica Et Traumatologica Turcica: H. Utkan Ayd In, Omer Berk OzanggiNoch keine Bewertungen
- In Search of A Better Equation - Performance and Equity in Estimates of Kidney FunctionDokument4 SeitenIn Search of A Better Equation - Performance and Equity in Estimates of Kidney FunctionanggiNoch keine Bewertungen
- Perspective: New England Journal MedicineDokument4 SeitenPerspective: New England Journal MedicineanggiNoch keine Bewertungen
- Middle Term Results of Tantalum Acetabular Cups in 2019 Acta Orthopaedica EtDokument5 SeitenMiddle Term Results of Tantalum Acetabular Cups in 2019 Acta Orthopaedica EtanggiNoch keine Bewertungen
- Mid Term Results With An Anatomic Stemless Shoulde 2019 Acta Orthopaedica EtDokument5 SeitenMid Term Results With An Anatomic Stemless Shoulde 2019 Acta Orthopaedica EtanggiNoch keine Bewertungen
- Psychometrical Properties of The Turkish Transla 2019 Acta Orthopaedica Et TDokument5 SeitenPsychometrical Properties of The Turkish Transla 2019 Acta Orthopaedica Et TanggiNoch keine Bewertungen
- Acta Orthopaedica Et Traumatologica Turcica: H. Utkan Ayd In, Omer Berk OzDokument3 SeitenActa Orthopaedica Et Traumatologica Turcica: H. Utkan Ayd In, Omer Berk OzanggiNoch keine Bewertungen
- Acta Orthopaedica Et Traumatologica Turcica: Cemil Ozal, Gonca Ari, Mintaze Kerem GunelDokument4 SeitenActa Orthopaedica Et Traumatologica Turcica: Cemil Ozal, Gonca Ari, Mintaze Kerem GunelanggiNoch keine Bewertungen
- Gastrointestinal Nursing Volume 7 Issue 1 2009 (Doi 10.12968/gasn.2009.7.1.39369) Cox, Carol Steggall, Martin - A Step By-Step Guide To Performing A Complete Abdominal ExaminationDokument7 SeitenGastrointestinal Nursing Volume 7 Issue 1 2009 (Doi 10.12968/gasn.2009.7.1.39369) Cox, Carol Steggall, Martin - A Step By-Step Guide To Performing A Complete Abdominal ExaminationanggiNoch keine Bewertungen
- Superficial Radial Nerve Compression Due To Fibrom 2019 Acta Orthopaedica EtDokument3 SeitenSuperficial Radial Nerve Compression Due To Fibrom 2019 Acta Orthopaedica EtanggiNoch keine Bewertungen
- Mechanical Properties and Morphologic Features of Int 2019 Acta OrthopaedicaDokument5 SeitenMechanical Properties and Morphologic Features of Int 2019 Acta OrthopaedicaanggiNoch keine Bewertungen
- Nej MSR 1707974Dokument5 SeitenNej MSR 1707974anggiNoch keine Bewertungen
- Nej MP 1705348Dokument3 SeitenNej MP 1705348anggiNoch keine Bewertungen
- A Woman Considering Contralateral Prophylactic MastectomyDokument4 SeitenA Woman Considering Contralateral Prophylactic MastectomyanggiNoch keine Bewertungen
- Nej Mic M 1703542Dokument1 SeiteNej Mic M 1703542anggiNoch keine Bewertungen
- Nej MC 1710384Dokument3 SeitenNej MC 1710384anggiNoch keine Bewertungen
- AB - Cube Vigilance Software SolutionsDokument2 SeitenAB - Cube Vigilance Software SolutionsKumar KumarNoch keine Bewertungen
- Sophisticated InstrumentationDokument3 SeitenSophisticated InstrumentationAnkit PatelNoch keine Bewertungen
- Ciprofloxacin: Supervisedby: DR - Ali Salama Done By: A T H A L A H M A D 2 0 2 0 1 0 3 3 9Dokument10 SeitenCiprofloxacin: Supervisedby: DR - Ali Salama Done By: A T H A L A H M A D 2 0 2 0 1 0 3 3 9wasan mousaNoch keine Bewertungen
- PhenobarbitalDokument3 SeitenPhenobarbitalChristine Joy Pepito50% (2)
- Ayurved Question PaperDokument8 SeitenAyurved Question Paperchauhan_892277982Noch keine Bewertungen
- Bafer Stok PKM 2015 AprilDokument16 SeitenBafer Stok PKM 2015 AprilMinarni KuraisNoch keine Bewertungen
- UntitledDokument137 SeitenUntitledSsaidsafa SaidNoch keine Bewertungen
- Drug ErrorsDokument25 SeitenDrug ErrorskordapyaisinthehouseNoch keine Bewertungen
- GlenmarkDokument11 SeitenGlenmarkpdkolkata1985Noch keine Bewertungen
- K CPP Ric List 251120Dokument230 SeitenK CPP Ric List 251120HarshaNoch keine Bewertungen
- Introduction To Microbiology: by T. Topodzi Bpharm (Hons) University of ZimbabweDokument13 SeitenIntroduction To Microbiology: by T. Topodzi Bpharm (Hons) University of ZimbabweVon Valentine MhuteNoch keine Bewertungen
- Studies On Enhancement Of Solubility And Dissolution Rate Of Ritonavir Employing Β-Cyclodextrin, Soluplus And Pvpk30Dokument11 SeitenStudies On Enhancement Of Solubility And Dissolution Rate Of Ritonavir Employing Β-Cyclodextrin, Soluplus And Pvpk30dini hanifaNoch keine Bewertungen
- CV Ak - 1502 - eDokument9 SeitenCV Ak - 1502 - evjeevan5Noch keine Bewertungen
- Roscacea JournalDokument5 SeitenRoscacea JournalanwarNoch keine Bewertungen
- FIBONACCIDokument5 SeitenFIBONACCIdrmukul5439Noch keine Bewertungen
- Medication Adherence PDFDokument11 SeitenMedication Adherence PDFAnonymous nuVdtDGTEtNoch keine Bewertungen
- DR - Harish DurejaDokument26 SeitenDR - Harish Durejaarpita_949242356Noch keine Bewertungen
- Nutraceutical Market ReportDokument22 SeitenNutraceutical Market ReportAmit SakpalNoch keine Bewertungen
- Standard Operating Procedure Cold Chain ManagementDokument3 SeitenStandard Operating Procedure Cold Chain ManagementDaniel Yves IV Paez100% (1)
- 10.1007@978 3 319 59542 9Dokument309 Seiten10.1007@978 3 319 59542 9Josué VelázquezNoch keine Bewertungen
- Interview With Barbara Loe Fisher On IOM Report 2011Dokument11 SeitenInterview With Barbara Loe Fisher On IOM Report 2011Fadhli QuzwainNoch keine Bewertungen
- Dyspepsia in PregnancyDokument1 SeiteDyspepsia in Pregnancydownload spssNoch keine Bewertungen
- Isolation of ProteinsDokument5 SeitenIsolation of ProteinscrayonNoch keine Bewertungen
- Nitrates Comparison ChartDokument7 SeitenNitrates Comparison ChartModi Evana PutriNoch keine Bewertungen
- SAS Projects DiscriptionDokument2 SeitenSAS Projects DiscriptionRavi Prakash MayreddyNoch keine Bewertungen
- Quality Control/Assurance ManagerDokument2 SeitenQuality Control/Assurance Managerapi-77569194Noch keine Bewertungen
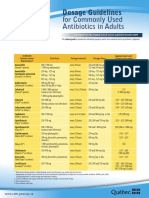
- CDM Antibio1 DosageGuidelines Adults enDokument2 SeitenCDM Antibio1 DosageGuidelines Adults endwiNoch keine Bewertungen
- Transition of CareDokument52 SeitenTransition of CareAffan PresentationsNoch keine Bewertungen
- Anaesthetic Drugs Cheat SheetsDokument2 SeitenAnaesthetic Drugs Cheat SheetsPkern100% (3)
- Pharmacology - Respiratory DrugsDokument61 SeitenPharmacology - Respiratory DrugsBenjamin Joel Breboneria100% (5)