Das könnte Ihnen auch gefallen
- Biomarcadores en IRC Temprana en Gatos 2013Dokument6 SeitenBiomarcadores en IRC Temprana en Gatos 2013Wilson Enrique Guerrero JojoaNoch keine Bewertungen
- Viswanathan2011 PDFDokument6 SeitenViswanathan2011 PDFRennilia NitaNoch keine Bewertungen
- Glomerulonefritis Primaria Medicine 2015Dokument6 SeitenGlomerulonefritis Primaria Medicine 2015Francisco Rebollar GarduñoNoch keine Bewertungen
- IsbelDokument7 SeitenIsbelCaity YoungNoch keine Bewertungen
- Viteri2018 Prevalensi 5Dokument17 SeitenViteri2018 Prevalensi 5adrian revoNoch keine Bewertungen
- Proteinuria in Diabetic Kidney Disease A MechanisticDokument15 SeitenProteinuria in Diabetic Kidney Disease A Mechanisticmutiara nurzaniNoch keine Bewertungen
- Flores - TVTDokument9 SeitenFlores - TVTChristian De LeonNoch keine Bewertungen
- Serum and Urine Biomarkers of Kidney Disease.Dokument8 SeitenSerum and Urine Biomarkers of Kidney Disease.Andronic GeorgeNoch keine Bewertungen
- Acute GlomerulonephritisDokument1 SeiteAcute GlomerulonephritisAyrheen FornolesNoch keine Bewertungen
- Proteinuria 1Dokument4 SeitenProteinuria 1Ledira Dara IsmiNoch keine Bewertungen
- Pancreatitis 1Dokument8 SeitenPancreatitis 1Romina GonzálezNoch keine Bewertungen
- Buletin DBDDokument8 SeitenBuletin DBDLedira Dara IsmiNoch keine Bewertungen
- Glomerulopatías PrimariasDokument8 SeitenGlomerulopatías PrimariasGSENoch keine Bewertungen
- 1 s2.0 S187952261200053X MainDokument8 Seiten1 s2.0 S187952261200053X MainRobert ChristevenNoch keine Bewertungen
- Henry's Clinical Diagnosis and Management by Laboratory Methods Twenty-Third Edition 2017Dokument20 SeitenHenry's Clinical Diagnosis and Management by Laboratory Methods Twenty-Third Edition 2017Denise GuevaraNoch keine Bewertungen
- Protein Uri ADokument2 SeitenProtein Uri AAmelia PebriantiNoch keine Bewertungen
- Concise Review For Primary-Care Physicians: Evaluation of ProteinuriaDokument5 SeitenConcise Review For Primary-Care Physicians: Evaluation of ProteinuriaRomadhona KhoiriNoch keine Bewertungen
- Flgastro 2018 101102Dokument8 SeitenFlgastro 2018 101102carolina pulidoNoch keine Bewertungen
- Renal Tutorial 1Dokument38 SeitenRenal Tutorial 1luckyswiss7776848Noch keine Bewertungen
- The Laboratory Diagnosis of Feline Kidney DiseaseDokument7 SeitenThe Laboratory Diagnosis of Feline Kidney DiseaseCabinet VeterinarNoch keine Bewertungen
- Primary Care Approach To Proteinuria: Amir Said Alizadeh Naderi, MD, and Robert F. Reilly, MDDokument6 SeitenPrimary Care Approach To Proteinuria: Amir Said Alizadeh Naderi, MD, and Robert F. Reilly, MDDarian AngNoch keine Bewertungen
- Reviews: WNT/ Dysfunction in Proteinuric Kidney DiseaseDokument11 SeitenReviews: WNT/ Dysfunction in Proteinuric Kidney DiseaseAlberto Carlos Espinosa GaravitoNoch keine Bewertungen
- Oliguria NEJM PDFDokument5 SeitenOliguria NEJM PDFHeeyeon BaeNoch keine Bewertungen
- 1 s2.0 S1548559510001412 MainDokument11 Seiten1 s2.0 S1548559510001412 Mainibnu cacingNoch keine Bewertungen
- Chronic PancreatitisDokument8 SeitenChronic PancreatitisSanjaya SenevirathneNoch keine Bewertungen
- Artigotutoria PDFDokument12 SeitenArtigotutoria PDFZARA BATISTANoch keine Bewertungen
- Postobstructive Diuresis: Clinical ReviewDokument6 SeitenPostobstructive Diuresis: Clinical ReviewRara Aulia IINoch keine Bewertungen
- Management of Primary Biliary Cirrhosis: Enny EathcoteDokument9 SeitenManagement of Primary Biliary Cirrhosis: Enny EathcoteMurat HessesNoch keine Bewertungen
- Practical Guide To The Management of Acute Pancreatitis: George Goodchild, Manil Chouhan, Gavin J JohnsonDokument8 SeitenPractical Guide To The Management of Acute Pancreatitis: George Goodchild, Manil Chouhan, Gavin J JohnsonRene CordovaNoch keine Bewertungen
- ProteinuriaDokument1 SeiteProteinuriamutiara nurzaniNoch keine Bewertungen
- ProteinuriaDokument12 SeitenProteinuriaSaraswati Wulandari HartonoNoch keine Bewertungen
- Problems in Adherence To GuidelinesDokument8 SeitenProblems in Adherence To GuidelinesJ Eduardo Cázares MontañezNoch keine Bewertungen
- Connally2003 Lavado Peritoneal DiagnosticoDokument6 SeitenConnally2003 Lavado Peritoneal Diagnosticoandres silvaNoch keine Bewertungen
- 15-Structure, Not Just FunctionDokument3 Seiten15-Structure, Not Just Functionjeb faqNoch keine Bewertungen
- Efusi Pleura MaskellDokument10 SeitenEfusi Pleura MaskellYessica Chrystie Dian SinurayaNoch keine Bewertungen
- How To Evaluate Dipstick Hematuria CCJM 2008Dokument7 SeitenHow To Evaluate Dipstick Hematuria CCJM 2008CANELO_PIANONoch keine Bewertungen
- Review and Update of Benign PRDokument6 SeitenReview and Update of Benign PRAgung KaryawinaraNoch keine Bewertungen
- Serum and Bile Biomarkers For Cholangiocarcinoma.19Dokument6 SeitenSerum and Bile Biomarkers For Cholangiocarcinoma.19asasasNoch keine Bewertungen
- Disorders of PancreasDokument17 SeitenDisorders of PancreasjonasNoch keine Bewertungen
- Pathobiology of Liver Fibrosis: A Translational Success StoryDokument13 SeitenPathobiology of Liver Fibrosis: A Translational Success StoryNovita ApramadhaNoch keine Bewertungen
- AJGP 2018 0102 Clinical CoeliacDokument6 SeitenAJGP 2018 0102 Clinical CoeliacAngie Viquez BeitaNoch keine Bewertungen
- Kidney Aging Sullivan 2016Dokument14 SeitenKidney Aging Sullivan 2016Doni Andika PutraNoch keine Bewertungen
- Clinical Pharmacy Nephrotic Syndrome: ChildrenDokument2 SeitenClinical Pharmacy Nephrotic Syndrome: ChildrenKristine AbrahamNoch keine Bewertungen
- Histopathology of Crohn's Disease and Ulcerative Colitis: Section 3Dokument22 SeitenHistopathology of Crohn's Disease and Ulcerative Colitis: Section 3HumoraNoch keine Bewertungen
- 1 s2.0 S0039914020310092 MainDokument20 Seiten1 s2.0 S0039914020310092 MainBen DresimNoch keine Bewertungen
- Chapter 3Dokument39 SeitenChapter 3hedieh abedNoch keine Bewertungen
- Topic 3Dokument17 SeitenTopic 3Jacqueline Tungcul DonatoNoch keine Bewertungen
- Is The Renal Biopsy Still Necessary in Lupus Nephropathy?Dokument4 SeitenIs The Renal Biopsy Still Necessary in Lupus Nephropathy?Hosne araNoch keine Bewertungen
- Coursebook-Biliary ch04Dokument19 SeitenCoursebook-Biliary ch04Daniela CioboataNoch keine Bewertungen
- Revarsate PleuraleDokument38 SeitenRevarsate PleuraleRaluca OpreaNoch keine Bewertungen
- Renal BiopsyDokument4 SeitenRenal BiopsyDeshan AdikariNoch keine Bewertungen
- Proteinuria in ChildrenDokument10 SeitenProteinuria in ChildrenabanvandiegoNoch keine Bewertungen
- Proteinuria During Pregnancy: Definition, Pathophysiology, Methodology, and Clinical SignificanceDokument16 SeitenProteinuria During Pregnancy: Definition, Pathophysiology, Methodology, and Clinical SignificanceJesi Anggraini Ekaputri LubisNoch keine Bewertungen
- Nefrotik SyndDokument13 SeitenNefrotik SyndJorianditha RamadhanNoch keine Bewertungen
- Lasificación Histopatológica de La Glomerulonefritis Asociada A ANCADokument9 SeitenLasificación Histopatológica de La Glomerulonefritis Asociada A ANCASaid SanchezNoch keine Bewertungen
- Current Concepts: Review ArticlesDokument6 SeitenCurrent Concepts: Review ArticlesEdgar VasquezNoch keine Bewertungen
- Autoimmune HepatitisDokument15 SeitenAutoimmune HepatitisAbudhoNoch keine Bewertungen
- Simplified Algorithm For Evaluation of Proteinuria in Clinical Practice: How Should A Clinician Approach?Dokument5 SeitenSimplified Algorithm For Evaluation of Proteinuria in Clinical Practice: How Should A Clinician Approach?Danny JacobusNoch keine Bewertungen
- Clinical Management: Chronic DiarrheaDokument7 SeitenClinical Management: Chronic DiarrheaAnonymous ce3S6XFdwUNoch keine Bewertungen
- Patogenesis IMNDokument23 SeitenPatogenesis IMNshiloinNoch keine Bewertungen
- SaudiJKidneyDisTranspl22110-3529284 094812Dokument8 SeitenSaudiJKidneyDisTranspl22110-3529284 094812shiloinNoch keine Bewertungen
- Steroid-Dependent Nephrotic SyndromeDokument34 SeitenSteroid-Dependent Nephrotic SyndromevkhrishikeshmenonNoch keine Bewertungen
- Midazolam in J PfizerDokument13 SeitenMidazolam in J PfizershiloinNoch keine Bewertungen
- Moyamoya Epidemiology, Presentation, and DiagnosisDokument9 SeitenMoyamoya Epidemiology, Presentation, and DiagnosisshiloinNoch keine Bewertungen
- Atopy in NSDokument13 SeitenAtopy in NSshiloinNoch keine Bewertungen
- Nagoya and Vicinity: Practical Travel Guide - 411Dokument5 SeitenNagoya and Vicinity: Practical Travel Guide - 411shiloinNoch keine Bewertungen
- Jonan Do Ri: Johoku DoriDokument4 SeitenJonan Do Ri: Johoku DorishiloinNoch keine Bewertungen
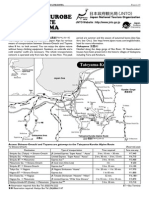
- Tateyama-Kurobe Alpine Route and GokayamaDokument4 SeitenTateyama-Kurobe Alpine Route and GokayamashiloinNoch keine Bewertungen
- Antique FleamarketsintokyoDokument2 SeitenAntique FleamarketsintokyoshiloinNoch keine Bewertungen
- Corticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisDokument7 SeitenCorticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisshiloinNoch keine Bewertungen
- Travel in Japan in More Convenient and Comfortable Ways: Up-To-Date Guide For Japan S Tourist EnvironmentDokument6 SeitenTravel in Japan in More Convenient and Comfortable Ways: Up-To-Date Guide For Japan S Tourist EnvironmentshiloinNoch keine Bewertungen
- Cvs-k7-Valvular Heart Disease Nora2010Dokument52 SeitenCvs-k7-Valvular Heart Disease Nora2010shiloinNoch keine Bewertungen
- Reflotron Plus Information BookletDokument28 SeitenReflotron Plus Information BookletKo Phyo WaiNoch keine Bewertungen
- Anemia in CKDDokument149 SeitenAnemia in CKDUlises ContrerasNoch keine Bewertungen
- RN Notes Med SurgDokument15 SeitenRN Notes Med Surgiamdarn100% (3)
- Hiperpotasemia KDIGODokument20 SeitenHiperpotasemia KDIGOAndy MaciasNoch keine Bewertungen
- Required: Body System: Session Topic: Educational Format Faculty Expertise RequiredDokument16 SeitenRequired: Body System: Session Topic: Educational Format Faculty Expertise RequiredThaysa LimaNoch keine Bewertungen
- Chronic Kidney DiseaseDokument36 SeitenChronic Kidney Diseasejabir100% (1)
- A 90-Day Subchronic Toxicity Study of Neem Oil, A Azadirachta Indica Oil, in MiceDokument11 SeitenA 90-Day Subchronic Toxicity Study of Neem Oil, A Azadirachta Indica Oil, in Micehenry72Noch keine Bewertungen
- Comprehensive Pharmacology Study NotesDokument123 SeitenComprehensive Pharmacology Study NotesEdil M Jama100% (1)
- 1 Pag 3Dokument14 Seiten1 Pag 3Mr. LNoch keine Bewertungen
- Covifor Serbuk Injeksi Liofilisasi 100 MG - Remdesivir - T-RG.01.03.32.322.09.20.04984, NE - 2020 PDFDokument22 SeitenCovifor Serbuk Injeksi Liofilisasi 100 MG - Remdesivir - T-RG.01.03.32.322.09.20.04984, NE - 2020 PDFHeru Joko SantosoNoch keine Bewertungen
- VHDL HighDokument302 SeitenVHDL HighsamNoch keine Bewertungen
- Multiple Oral Dose Administration 30maioDokument27 SeitenMultiple Oral Dose Administration 30maiovenkateshyadav21160% (1)
- C. Case Study thesis-NCP (Revised)Dokument5 SeitenC. Case Study thesis-NCP (Revised)Lopirts NiganiNoch keine Bewertungen
- FebuxostatDokument14 SeitenFebuxostatSanjay NavaleNoch keine Bewertungen
- Effects of Creatine Supplementation On Renal Function - A Systematic Review and Meta-AnalysisDokument10 SeitenEffects of Creatine Supplementation On Renal Function - A Systematic Review and Meta-AnalysisNaiara CaramuruNoch keine Bewertungen
- Doctor's OrderDokument3 SeitenDoctor's OrderStephen S. PadayhagNoch keine Bewertungen
- Clinical Guideline: Aminoglycoside: Recommendations For Use, Dosing and Monitoring Clinical GuidelineDokument16 SeitenClinical Guideline: Aminoglycoside: Recommendations For Use, Dosing and Monitoring Clinical GuidelineVita LesielaNoch keine Bewertungen
- NonProteinNitrogen WorksheetDokument27 SeitenNonProteinNitrogen WorksheetMaria ClaraNoch keine Bewertungen
- Drugs in Palliative CareDokument593 SeitenDrugs in Palliative Carejulio.testi698295Noch keine Bewertungen
- Vec TrineDokument3 SeitenVec TrinerwdNoch keine Bewertungen
- Gap Assessment For Laboratory Development CMLS - SL (BOOK 1)Dokument28 SeitenGap Assessment For Laboratory Development CMLS - SL (BOOK 1)Ravi KumudeshNoch keine Bewertungen
- Clinical Data Zeftrax-SDokument37 SeitenClinical Data Zeftrax-SSem.Jb Tan0% (1)
- Function of The Renal and Urinary Tract System: Medical-Surgical Nursing, 4/eDokument117 SeitenFunction of The Renal and Urinary Tract System: Medical-Surgical Nursing, 4/eBryJos tiongsonNoch keine Bewertungen
- Exam 2 STUDY GUIDEDokument121 SeitenExam 2 STUDY GUIDEJulie BrandtNoch keine Bewertungen
- Obectives of Case Study: General ObjectivesDokument42 SeitenObectives of Case Study: General Objectivesganesh0% (1)
- 2017 Kdigo LD GL PDFDokument115 Seiten2017 Kdigo LD GL PDFBayu Triguna0% (1)
- Gagal Ginjal Kuliah FarmakoterapiDokument39 SeitenGagal Ginjal Kuliah FarmakoterapiriyuNoch keine Bewertungen
- DietaDokument32 SeitenDietaEve PeciNoch keine Bewertungen
- EDTA Chelation Therapy ArticlesDokument46 SeitenEDTA Chelation Therapy ArticlesBhalchandra Gokhale100% (1)
- Medicine June 2009: Fcps Part1 Q BankDokument14 SeitenMedicine June 2009: Fcps Part1 Q Bankqudsia_niaziNoch keine Bewertungen