Das könnte Ihnen auch gefallen
- Effect of endodontic sealers on bond strength of restorative systems to primary tooth pulp chamberDokument9 SeitenEffect of endodontic sealers on bond strength of restorative systems to primary tooth pulp chamberTiffany ArdhianaNoch keine Bewertungen
- Effect of endodontic sealers on bond strength of restorative systems to primary tooth pulp chamberDokument9 SeitenEffect of endodontic sealers on bond strength of restorative systems to primary tooth pulp chamberTiffany ArdhianaNoch keine Bewertungen
- Chilean Patients' Perception of Oral Health-Related Quality of Life After Third Molar SurgeryDokument7 SeitenChilean Patients' Perception of Oral Health-Related Quality of Life After Third Molar SurgeryTiffany ArdhianaNoch keine Bewertungen
- Alergi NikelDokument4 SeitenAlergi NikelTiffany ArdhianaNoch keine Bewertungen
- JCDR 9 ZC62Dokument3 SeitenJCDR 9 ZC62Tiffany ArdhianaNoch keine Bewertungen
- JurnalDokument5 SeitenJurnalFaiza LailiyahNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- New Patient Medical History FormDokument5 SeitenNew Patient Medical History FormSonuraj rana RanaNoch keine Bewertungen
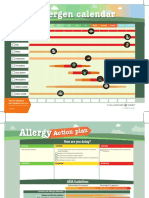
- Allergen Calendar - EnglishDokument2 SeitenAllergen Calendar - Englishpkgill15Noch keine Bewertungen
- AlerTox Sticks Soy PLUS ManualDokument8 SeitenAlerTox Sticks Soy PLUS ManualLuis Miguel Matos OteroNoch keine Bewertungen
- Screenshot 2022-09-29 at 12.13.10 PMDokument6 SeitenScreenshot 2022-09-29 at 12.13.10 PMgaalaxy ggNoch keine Bewertungen
- 1105 Welbrite SDS 20200307 New VersionDokument11 Seiten1105 Welbrite SDS 20200307 New VersiontinzarmoeNoch keine Bewertungen
- Allergic reactions to hair dye on the riseDokument2 SeitenAllergic reactions to hair dye on the riseSamy Abdulghaffar Mostafa Abul-ElaNoch keine Bewertungen
- Veterinary Acupuncture Book From Philip RogersDokument727 SeitenVeterinary Acupuncture Book From Philip Rogersadorjaan100% (3)
- Allergy Plex V-M enDokument62 SeitenAllergy Plex V-M enAlessandro Rossi100% (1)
- Allergy Voices Volume 2 CompressedDokument47 SeitenAllergy Voices Volume 2 CompressedHermiNoch keine Bewertungen
- Study of Regulatory Restrictions in The Field of PharmaciesDokument30 SeitenStudy of Regulatory Restrictions in The Field of PharmaciesAnonymous hF5zAdvwCCNoch keine Bewertungen
- Therapy PulmonologyDokument22 SeitenTherapy PulmonologyCavinpal SinghNoch keine Bewertungen
- A Review On Atopic Dermatitis Etiology, Clinical Features, Pathogenesis, Diagnosis, and Various TreatmentsDokument12 SeitenA Review On Atopic Dermatitis Etiology, Clinical Features, Pathogenesis, Diagnosis, and Various TreatmentsEditor IJTSRDNoch keine Bewertungen
- Health 7 Activity SheetsDokument31 SeitenHealth 7 Activity SheetsGABINO ELECTRONIC REPAIR & PRINTING SERVICESNoch keine Bewertungen
- Red MeatDokument9 SeitenRed Meatarka prava LahiriNoch keine Bewertungen
- Irritant Contact Dermatitis: Causes, Symptoms, TreatmentDokument13 SeitenIrritant Contact Dermatitis: Causes, Symptoms, TreatmentYoga Alfian NoorNoch keine Bewertungen
- PSAAI Position Statements on COVID-19 VaccinesDokument25 SeitenPSAAI Position Statements on COVID-19 VaccinesMonica LowinskiNoch keine Bewertungen
- CAE Reading and Use of English Practice Test 9 Printable-Các Trang Đã XóaDokument9 SeitenCAE Reading and Use of English Practice Test 9 Printable-Các Trang Đã Xóakaycharlie360Noch keine Bewertungen
- (ThichTiengAnh.Com) Đề 002 - PRO SAT 2017 PDFDokument12 Seiten(ThichTiengAnh.Com) Đề 002 - PRO SAT 2017 PDFNguyen Hiep DuyNoch keine Bewertungen
- Chapter37 Assessment and Management of Patients With Allergic DisordersDokument40 SeitenChapter37 Assessment and Management of Patients With Allergic Disordersjericho dinglasanNoch keine Bewertungen
- Contact Dermatitis: A Practice ParameterDokument38 SeitenContact Dermatitis: A Practice ParameterdhirazhrNoch keine Bewertungen
- Antihistamine in Pediatrics AllergyDokument10 SeitenAntihistamine in Pediatrics AllergyIndra AdjuddinNoch keine Bewertungen
- Surgery For Allergic Rhinitis Chhabra2014Dokument5 SeitenSurgery For Allergic Rhinitis Chhabra2014Gaby ToledoNoch keine Bewertungen
- Chronic UrticariaDokument4 SeitenChronic UrticariaayukNoch keine Bewertungen
- ASCIA HP Penicillin Allergy Guide 2016Dokument1 SeiteASCIA HP Penicillin Allergy Guide 2016kkkssbbNoch keine Bewertungen
- Food Allergy and IntoleranceDokument2 SeitenFood Allergy and IntoleranceShielaMaeTorinoPilisingNoch keine Bewertungen
- 2019 Medical Certificate1Dokument5 Seiten2019 Medical Certificate1lea bendijoNoch keine Bewertungen
- Hypersensitivity ReactionsDokument2 SeitenHypersensitivity ReactionsMythily VedhagiriNoch keine Bewertungen
- Anonymous - EOE Challenging Journey To Diagnosis - HCP LiveDokument4 SeitenAnonymous - EOE Challenging Journey To Diagnosis - HCP LiveGeorge LucasNoch keine Bewertungen
- 10 de Thi Thu Thpt Quoc Giamon Tieng Anh Co Dap an Giai Thich Chi Tiet 1 Đã Chuyển ĐổiDokument148 Seiten10 de Thi Thu Thpt Quoc Giamon Tieng Anh Co Dap an Giai Thich Chi Tiet 1 Đã Chuyển Đổilâm HoangNoch keine Bewertungen
- Asthma SOAP NoteDokument1 SeiteAsthma SOAP NoteRavi KiranNoch keine Bewertungen