Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Assignment On Diesel Engine OverhaulingDokument19 SeitenAssignment On Diesel Engine OverhaulingRuwan Susantha100% (3)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Risk Criteria - When Is Low Enough Good Enough - SaudiDokument8 SeitenRisk Criteria - When Is Low Enough Good Enough - Saudiuserscribd2011Noch keine Bewertungen
- Lab 7 RC Time ConstantDokument8 SeitenLab 7 RC Time ConstantMalith Madushan100% (1)
- Reflective Paper Assignment 2 Professional Practice Level 2Dokument3 SeitenReflective Paper Assignment 2 Professional Practice Level 2api-350779667Noch keine Bewertungen
- Jarratt Davis: How To Trade A Currency FundDokument5 SeitenJarratt Davis: How To Trade A Currency FundRui100% (1)
- SPONSORSHIP GUIDE FOR FIJI'S NATIONAL SPORTS FEDERATIONSDokument17 SeitenSPONSORSHIP GUIDE FOR FIJI'S NATIONAL SPORTS FEDERATIONSvaidwara100% (1)
- Typewriter Olivetti Linea98 SerManDokument66 SeitenTypewriter Olivetti Linea98 SerManmplennaNoch keine Bewertungen
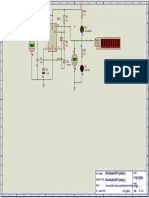
- Oscilador Baud Rate para 90HzDokument1 SeiteOscilador Baud Rate para 90HzmplennaNoch keine Bewertungen
- PW 1979 02Dokument93 SeitenPW 1979 02mplennaNoch keine Bewertungen
- AN555Dokument38 SeitenAN555Hernan Ortiz EnamoradoNoch keine Bewertungen
- Transformers - Alexander SchureDokument88 SeitenTransformers - Alexander SchuremplennaNoch keine Bewertungen
- Rider-Resonance and Alignment - John F. RiderDokument95 SeitenRider-Resonance and Alignment - John F. RidermplennaNoch keine Bewertungen
- KA2297 DatasheetDokument6 SeitenKA2297 DatasheetmplennaNoch keine Bewertungen
- 5.3W 2-Channel AF Power Amplifier: Package Dimensions FeaturesDokument12 Seiten5.3W 2-Channel AF Power Amplifier: Package Dimensions FeaturesmplennaNoch keine Bewertungen
- LongWave TransmitterDokument1 SeiteLongWave TransmittermplennaNoch keine Bewertungen
- Features Description: FM IF SystemDokument8 SeitenFeatures Description: FM IF Systemraan4Noch keine Bewertungen
- Ampl 15 WDokument1 SeiteAmpl 15 WmplennaNoch keine Bewertungen
- MC1310Dokument8 SeitenMC1310Ricardo MenzerNoch keine Bewertungen
- Ordering number EN1840A: LA1186N Monolithic Linear IC for FM Front EndsDokument5 SeitenOrdering number EN1840A: LA1186N Monolithic Linear IC for FM Front EndsmatiasNoch keine Bewertungen
- Radio Craft 33 Amplifier Builder's GuideDokument68 SeitenRadio Craft 33 Amplifier Builder's GuidemplennaNoch keine Bewertungen
- Radio TV Experimenter 1963 SpringDokument196 SeitenRadio TV Experimenter 1963 SpringmplennaNoch keine Bewertungen
- Radio TV Experimenter 1965-02-03Dokument132 SeitenRadio TV Experimenter 1965-02-03mplennaNoch keine Bewertungen
- Radio TV Experimenter 1963 SpringDokument196 SeitenRadio TV Experimenter 1963 SpringmplennaNoch keine Bewertungen
- Schematic Layout and Design GuideDokument69 SeitenSchematic Layout and Design GuideАндрей ФандеевNoch keine Bewertungen
- Fitch - The-Superheterodyne-BookDokument70 SeitenFitch - The-Superheterodyne-BookmplennaNoch keine Bewertungen
- Teachersmanualto 00 CollrichDokument56 SeitenTeachersmanualto 00 CollrichmplennaNoch keine Bewertungen
- Rins Piora Homocisteina AumentaDokument7 SeitenRins Piora Homocisteina AumentamplennaNoch keine Bewertungen
- Radio TV Experimenter 1957 Vol 4Dokument196 SeitenRadio TV Experimenter 1957 Vol 4mplennaNoch keine Bewertungen
- S I 4 8 2 2 / 2 6 / 2 7 / 4 0 / 4 4 A, S, L, D G: Ntenna Chematic Ayout AND Esign UidelinesDokument38 SeitenS I 4 8 2 2 / 2 6 / 2 7 / 4 0 / 4 4 A, S, L, D G: Ntenna Chematic Ayout AND Esign UidelinesmplennaNoch keine Bewertungen
- CD4020BC - CD4040BC - CD4060BC 14-Stage Ripple Carry Binary Counters - 12-Stage Ripple Carry Binary Counters - 14-Stage Ripple Carry Binary CountersDokument8 SeitenCD4020BC - CD4040BC - CD4060BC 14-Stage Ripple Carry Binary Counters - 12-Stage Ripple Carry Binary Counters - 14-Stage Ripple Carry Binary CountersmplennaNoch keine Bewertungen
- Babani 58 50 Circuits Using 7400 ICsDokument82 SeitenBabani 58 50 Circuits Using 7400 ICsmplennaNoch keine Bewertungen
- Si861x/2x Data Sheet: Low-Power Single and Dual-Channel Digital IsolatorsDokument39 SeitenSi861x/2x Data Sheet: Low-Power Single and Dual-Channel Digital IsolatorsmplennaNoch keine Bewertungen
- SI 4825 ReceptorDokument37 SeitenSI 4825 ReceptorLuis100% (1)
- B Am/Fm R R: Roadcast Adio EceiverDokument42 SeitenB Am/Fm R R: Roadcast Adio EceiverChobits PhamNoch keine Bewertungen
- Role of Vitamins D, E and C in Immunity and in AmmationDokument6 SeitenRole of Vitamins D, E and C in Immunity and in AmmationmplennaNoch keine Bewertungen
- G DFE G DFE: Main Functions Good SourcesDokument1 SeiteG DFE G DFE: Main Functions Good SourcesmplennaNoch keine Bewertungen
- Volleyball TermsDokument2 SeitenVolleyball TermskimmybapkiddingNoch keine Bewertungen
- Comparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 YearsDokument4 SeitenComparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 Yearsmanjula dangeNoch keine Bewertungen
- A Photograph Poem Summary in EnglishDokument6 SeitenA Photograph Poem Summary in Englishpappu kalaNoch keine Bewertungen
- FortiEDR Product Overview TrainingDokument16 SeitenFortiEDR Product Overview TrainingRafael Steven Soto del CampoNoch keine Bewertungen
- Technical and Cost Model For Slipway DevelopmentDokument36 SeitenTechnical and Cost Model For Slipway DevelopmentshahjadaNoch keine Bewertungen
- RUN ON SENTENCES AND FRAGMENTS GUIDEDokument17 SeitenRUN ON SENTENCES AND FRAGMENTS GUIDEWAHEED-UL -ISLAMNoch keine Bewertungen
- Present Tense Review for Motorcycle RepairDokument2 SeitenPresent Tense Review for Motorcycle RepairFaheemuddin Veterans50% (2)
- Sidak 2008 FAQsDokument3 SeitenSidak 2008 FAQssikhswimNoch keine Bewertungen
- The Bare Foot Boy 3 Ab 2 ManadoDokument100 SeitenThe Bare Foot Boy 3 Ab 2 ManadoKotakuNoch keine Bewertungen
- Kamala Das Poetry CollectionDokument0 SeitenKamala Das Poetry CollectionBasa SwaminathanNoch keine Bewertungen
- Corporate Insolvency NotesDokument15 SeitenCorporate Insolvency NotesAnirudh SoodNoch keine Bewertungen
- Case StudyDokument9 SeitenCase StudySidharth A.murabatteNoch keine Bewertungen
- 1.MIL 1. Introduction To MIL Part 2 Characteristics of Information Literate Individual and Importance of MILDokument24 Seiten1.MIL 1. Introduction To MIL Part 2 Characteristics of Information Literate Individual and Importance of MILBernadette MendozaNoch keine Bewertungen
- Lower and Upper Bound Theory ExplainedDokument37 SeitenLower and Upper Bound Theory ExplainedTsuki ZombinaNoch keine Bewertungen
- JIPMER B.Sc. Prospectus 2016Dokument31 SeitenJIPMER B.Sc. Prospectus 2016Curtis LawsonNoch keine Bewertungen
- Form 3: (See Rule 54 (12) ) Details of FamilyDokument1 SeiteForm 3: (See Rule 54 (12) ) Details of FamilySaikat SarkarNoch keine Bewertungen
- Fuentes CAED PortfolioDokument32 SeitenFuentes CAED PortfoliojsscabatoNoch keine Bewertungen
- Outlook Business The Boss July 2015Dokument14 SeitenOutlook Business The Boss July 2015Nibedita MahatoNoch keine Bewertungen
- Physics 5th Edition Walker Test BankDokument24 SeitenPhysics 5th Edition Walker Test BankKathyHernandeznobt100% (31)
- Organization and Workflow Management of Central ST PDFDokument5 SeitenOrganization and Workflow Management of Central ST PDFravsab GaikwadNoch keine Bewertungen
- IEEE COMMUNICATIONS LETTERS, VOL. 10, NO. 6, JUNE 2006Dokument3 SeitenIEEE COMMUNICATIONS LETTERS, VOL. 10, NO. 6, JUNE 2006Regina PittsNoch keine Bewertungen
- NystgmusDokument16 SeitenNystgmusCheska Justine San JuanNoch keine Bewertungen
- Paradine V Jane - (1646) 82 ER 897Dokument2 SeitenParadine V Jane - (1646) 82 ER 897TimishaNoch keine Bewertungen