Das könnte Ihnen auch gefallen
- Agueh Curriculum VitaeDokument3 SeitenAgueh Curriculum VitaeAlex SilvanoNoch keine Bewertungen
- HI Classmates!!!Dokument36 SeitenHI Classmates!!!Alex SilvanoNoch keine Bewertungen
- Infectious Disease Outbreaks and Increased Complexity of CareDokument9 SeitenInfectious Disease Outbreaks and Increased Complexity of CareAlex SilvanoNoch keine Bewertungen
- Construction Methods and Project Managements: (Pert/Cpm)Dokument1 SeiteConstruction Methods and Project Managements: (Pert/Cpm)tmskieNoch keine Bewertungen
- Anemia CompleteDokument84 SeitenAnemia CompleteAlex SilvanoNoch keine Bewertungen
- GordonsDokument83 SeitenGordonsAlex SilvanoNoch keine Bewertungen
- Clozapine Drug StudyDokument2 SeitenClozapine Drug StudyAlex Silvano100% (2)
- AbstractDokument3 SeitenAbstractAlex SilvanoNoch keine Bewertungen
- Drug Therapeutic RecordDokument4 SeitenDrug Therapeutic RecordAlex SilvanoNoch keine Bewertungen
- DTRDokument63 SeitenDTRAlex SilvanoNoch keine Bewertungen
- Status and Acceptability of The Concrete Gravity Dam in Culaba, BiliranDokument1 SeiteStatus and Acceptability of The Concrete Gravity Dam in Culaba, BiliranAlex SilvanoNoch keine Bewertungen
- PTBDokument3 SeitenPTBAlex SilvanoNoch keine Bewertungen
- Drug StudyDokument12 SeitenDrug StudyAlex Silvano0% (1)
- Physical AssessmenttDokument3 SeitenPhysical AssessmenttAlex SilvanoNoch keine Bewertungen
- Nursing Care Plan Cues Nursing Diagnosis Scientific Analysis Objectives Nursing Interventions Rationale Evaluat IONDokument6 SeitenNursing Care Plan Cues Nursing Diagnosis Scientific Analysis Objectives Nursing Interventions Rationale Evaluat IONAlex SilvanoNoch keine Bewertungen
- Nursing Care Plan Cues Nursing Diagnosis Scientific Analysis Objectives Nursing Interventions Rationale Evaluat IONDokument6 SeitenNursing Care Plan Cues Nursing Diagnosis Scientific Analysis Objectives Nursing Interventions Rationale Evaluat IONAlex SilvanoNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Brucellosis Brucellosis: Brucella Spp. Brucella SPPDokument24 SeitenBrucellosis Brucellosis: Brucella Spp. Brucella SPPhussain AltaherNoch keine Bewertungen
- Benign Breast DiseasesDokument35 SeitenBenign Breast DiseasesBhim Nath KharelNoch keine Bewertungen
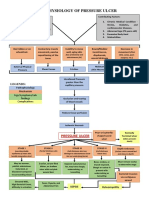
- Pathophysiology of Pressure UlcerDokument1 SeitePathophysiology of Pressure UlcerSTORAGE FILENoch keine Bewertungen
- Infectious DiseaseDokument6 SeitenInfectious DiseaseJoshua AjomNoch keine Bewertungen
- ECG Crib SheetDokument2 SeitenECG Crib Sheetkp180surfingNoch keine Bewertungen
- Prevenção Secundária Avc Isquêmico - Guideline 2022Dokument41 SeitenPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuNoch keine Bewertungen
- Vigabatrin For IsDokument12 SeitenVigabatrin For IsAndrew SantosoNoch keine Bewertungen
- Neonatal Respiratory DistressDokument59 SeitenNeonatal Respiratory DistressMohamad Saleh100% (7)
- Acetylcholine Esterase AntibodyDokument2 SeitenAcetylcholine Esterase AntibodySrinivasanNoch keine Bewertungen
- Valvular Heart DiseaseDokument73 SeitenValvular Heart Diseaseindia2puppy100% (4)
- Data Lens Overview: Category Keyword CountDokument25 SeitenData Lens Overview: Category Keyword CountHari HaranNoch keine Bewertungen
- NCM 104 RLE Module 3 FinalsDokument22 SeitenNCM 104 RLE Module 3 FinalsAlexander DontonNoch keine Bewertungen
- Case Study On Nephrotic SyndromeDokument7 SeitenCase Study On Nephrotic SyndromeArchana VermaNoch keine Bewertungen
- "Oral Questions in Clinical Surgery" Case 1. LipomaDokument19 Seiten"Oral Questions in Clinical Surgery" Case 1. LipomaSherif Magdi100% (3)
- Full-Sentence Speech FinalDokument2 SeitenFull-Sentence Speech Finalapi-363883917Noch keine Bewertungen
- Assignment 1 Part 1 A1Dokument10 SeitenAssignment 1 Part 1 A1garrenaNoch keine Bewertungen
- Assessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentDokument3 SeitenAssessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentKim Glaidyl BontuyanNoch keine Bewertungen
- Removal of Impacted Third MolarDokument13 SeitenRemoval of Impacted Third MolarHarkanNoch keine Bewertungen
- Wellen EcgDokument9 SeitenWellen EcgElokNoch keine Bewertungen
- NCP (Diarrhea)Dokument2 SeitenNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Proton Pump Inhibitors, Adverse Events and Increased Risk of MortalityDokument36 SeitenProton Pump Inhibitors, Adverse Events and Increased Risk of MortalityMohammad Mahmudur RahmanNoch keine Bewertungen
- Normal Digestion / Absorption of FatDokument5 SeitenNormal Digestion / Absorption of FatMarc Michael Dela CruzNoch keine Bewertungen
- Nursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of NursingDokument3 SeitenNursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of NursingZedoo AlmaroaaneNoch keine Bewertungen
- Syphilis Symptoms, Causes, and DiagnosisDokument3 SeitenSyphilis Symptoms, Causes, and DiagnosisIndra FahleviNoch keine Bewertungen
- Non-Sickle HB Variants.091611Dokument44 SeitenNon-Sickle HB Variants.091611Sumihar PasaribuNoch keine Bewertungen
- THC AspergerDokument168 SeitenTHC AspergerMICHAELNoch keine Bewertungen
- Hallucinations: Clinical Aspects and Management: Industrial Psychiatry Journal February 2020Dokument10 SeitenHallucinations: Clinical Aspects and Management: Industrial Psychiatry Journal February 2020Nyong FenNoch keine Bewertungen
- Community Medicine Notes & Question Bank: MBBS para ClinicalDokument67 SeitenCommunity Medicine Notes & Question Bank: MBBS para ClinicalAnish Nazar100% (2)
- Answers Mock Exam 1Dokument8 SeitenAnswers Mock Exam 1Amin AzadNoch keine Bewertungen
- Implanted Venous Access Device (IVAD) - "Dome" or "Port"Dokument12 SeitenImplanted Venous Access Device (IVAD) - "Dome" or "Port"JunkNoch keine Bewertungen