Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Treatment of Diabetic Neuropathy - UpToDateDokument20 SeitenTreatment of Diabetic Neuropathy - UpToDateKarina MilaréNoch keine Bewertungen
- Sample of A Critical Analysis of An ArticleDokument3 SeitenSample of A Critical Analysis of An ArticleGayle Thorne-cNoch keine Bewertungen
- Opioid-Free AnesthesiaDokument8 SeitenOpioid-Free AnesthesiaPaulina LugoNoch keine Bewertungen
- Chapter 34. Pain Management, Self-Assessment QuestionsDokument7 SeitenChapter 34. Pain Management, Self-Assessment Questionstsegaab yosephNoch keine Bewertungen
- Pharma Handouts Rev 3Dokument34 SeitenPharma Handouts Rev 3Aphrill Pearl PacisNoch keine Bewertungen
- Fentanyl Advisory Manufacturing Tab A 508Dokument13 SeitenFentanyl Advisory Manufacturing Tab A 508BrianNoch keine Bewertungen
- Substance AbuseDokument8 SeitenSubstance Abuseapi-19780865Noch keine Bewertungen
- Local Anesthetics, IV Sedation and Pain ManagementDokument70 SeitenLocal Anesthetics, IV Sedation and Pain ManagementHosam GomaaNoch keine Bewertungen
- Cannabis - 650 Current Peer Reviewed ReportsDokument762 SeitenCannabis - 650 Current Peer Reviewed ReportsJeffPrager100% (1)
- Osa DR S S FazalDokument92 SeitenOsa DR S S FazalAparup SaluiNoch keine Bewertungen
- Pil 7666Dokument8 SeitenPil 7666Paskalis HarrisNoch keine Bewertungen
- Unit 5 Basic Care and Comfort & Infection ControlDokument4 SeitenUnit 5 Basic Care and Comfort & Infection ControlAlyssa GarrettNoch keine Bewertungen
- Histamine and AntihistaminesDokument14 SeitenHistamine and AntihistaminesTrishaRaquepoNoch keine Bewertungen
- Document DRUG 4Dokument4 SeitenDocument DRUG 4Linda AdamsonNoch keine Bewertungen
- QN Paper Topic Wise .2 PDFDokument132 SeitenQN Paper Topic Wise .2 PDFDrLalit Kumar SamantarayNoch keine Bewertungen
- Trust FormularyDokument345 SeitenTrust Formularygiormarino2483Noch keine Bewertungen
- Drug Study..DokcyDokument7 SeitenDrug Study..DokcyPeArl Peralta0% (1)
- Shivering and Neuraxial AnesthesiaDokument12 SeitenShivering and Neuraxial AnesthesiaKarla Albert ReyesNoch keine Bewertungen
- Magnitude Substance Use India REPORT PDFDokument87 SeitenMagnitude Substance Use India REPORT PDFSarath KvNoch keine Bewertungen
- Drug Acting On Immune SystemDokument7 SeitenDrug Acting On Immune SystemAnne Giselle PatocNoch keine Bewertungen
- Pharmacological Studies On 7-Hydroxymitragynine, Isolated From The Thai Herbal Medicine Mitragyna Speciosa: Discovery of An Orally Active Opioid AnalgesicDokument85 SeitenPharmacological Studies On 7-Hydroxymitragynine, Isolated From The Thai Herbal Medicine Mitragyna Speciosa: Discovery of An Orally Active Opioid Analgesicjmp992100% (1)
- Guidelines For Managing Substance Withdrawal in JailsDokument128 SeitenGuidelines For Managing Substance Withdrawal in JailsepraetorianNoch keine Bewertungen
- ParacetamolDokument12 SeitenParacetamolAbhinav JayaramanNoch keine Bewertungen
- Osteoarthritis of The Hip: Clinical PracticeDokument9 SeitenOsteoarthritis of The Hip: Clinical PracticeMarina Tomasenco - DaniciNoch keine Bewertungen
- Sample: Reading Sub-Test - Question Paper: Part ADokument24 SeitenSample: Reading Sub-Test - Question Paper: Part ADr. Emad Elbadawy د عماد البدويNoch keine Bewertungen
- Neurobiology of Addiction PDFDokument6 SeitenNeurobiology of Addiction PDFAriol ZereNoch keine Bewertungen
- The Efficacy of Combination Analgesic Therapy in Relieving Dental PainDokument11 SeitenThe Efficacy of Combination Analgesic Therapy in Relieving Dental Painjosselyn berrioNoch keine Bewertungen
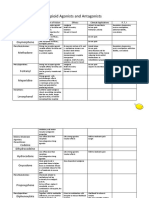
- Opioid Agonists and AntagonistsDokument5 SeitenOpioid Agonists and AntagonistsCas BuNoch keine Bewertungen
- AmphetamineDokument87 SeitenAmphetamineSATYABBSR83% (12)
- Drug AbuseDokument77 SeitenDrug AbuseEmilioNoch keine Bewertungen