Das könnte Ihnen auch gefallen
- HSE MAC Tool PDFDokument15 SeitenHSE MAC Tool PDFbeddows_sNoch keine Bewertungen
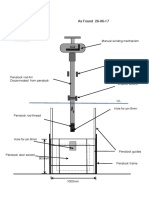
- As Found Survey - PenstockDokument1 SeiteAs Found Survey - Penstockbeddows_sNoch keine Bewertungen
- HSE MAC Tool PDFDokument15 SeitenHSE MAC Tool PDFbeddows_sNoch keine Bewertungen
- Airlift UsageDokument1 SeiteAirlift Usagebeddows_sNoch keine Bewertungen
- ICO - Registration FormDokument1 SeiteICO - Registration Formbeddows_sNoch keine Bewertungen
- 3817 Guidance NotesDokument3 Seiten3817 Guidance Notesbeddows_sNoch keine Bewertungen
- 2015 PTS Directory BookDokument270 Seiten2015 PTS Directory Bookbeddows_sNoch keine Bewertungen
- NORSOK Standard U-102Dokument46 SeitenNORSOK Standard U-102cristianoclemNoch keine Bewertungen
- HSE Policy Poster 1 July 2012Dokument1 SeiteHSE Policy Poster 1 July 2012beddows_sNoch keine Bewertungen
- Start Fittness T&C'sDokument4 SeitenStart Fittness T&C'sbeddows_sNoch keine Bewertungen
- Dart Fisher OffshoreSupportVesselDokument8 SeitenDart Fisher OffshoreSupportVesselbeddows_sNoch keine Bewertungen
- Lecture 4 Slabs - Oct 12 - EndDokument131 SeitenLecture 4 Slabs - Oct 12 - EndajayNoch keine Bewertungen
- Start Fittness FAQDokument4 SeitenStart Fittness FAQbeddows_sNoch keine Bewertungen
- L148 Safety in DocksDokument64 SeitenL148 Safety in Docksbeddows_sNoch keine Bewertungen
- Lecture 5 FoundationsDokument44 SeitenLecture 5 Foundationsbeddows_sNoch keine Bewertungen
- Lecture 5 FoundationsDokument44 SeitenLecture 5 Foundationsbeddows_sNoch keine Bewertungen
- 737 Form Cashback 150-500mmDokument1 Seite737 Form Cashback 150-500mmbeddows_sNoch keine Bewertungen
- Good Slipway DesignDokument4 SeitenGood Slipway Designbeddows_s100% (1)
- ICE3000 Development Objectives for Engineering ProjectsDokument1 SeiteICE3000 Development Objectives for Engineering Projectsbeddows_sNoch keine Bewertungen
- 3424 001Dokument8 Seiten3424 001beddows_sNoch keine Bewertungen
- Lecture 2 Beams - Concrete CenterDokument99 SeitenLecture 2 Beams - Concrete Centerwanksta67Noch keine Bewertungen
- How To Design Concrete Structures To EuroCode 2Dokument117 SeitenHow To Design Concrete Structures To EuroCode 2beddows_s100% (4)
- 2 CirclesDokument1 Seite2 Circlesbeddows_sNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Relieve Allergic Conjunctivitis Eyes NaturallyDokument2 SeitenRelieve Allergic Conjunctivitis Eyes NaturallyvichavkNoch keine Bewertungen
- Safer Oral Sex BrochureDokument2 SeitenSafer Oral Sex BrochureAugustin SekhemAset MureseanuNoch keine Bewertungen
- Obat Keras Harga Barang TotalDokument18 SeitenObat Keras Harga Barang Totalkhadifa dwiNoch keine Bewertungen
- Meropenem Drug StudyDokument2 SeitenMeropenem Drug StudyPhoebe Guevarra100% (8)
- Project Excel Kap DataDokument45 SeitenProject Excel Kap DataDHIVYANoch keine Bewertungen
- HHS DM Tipe 2Dokument39 SeitenHHS DM Tipe 2Rizki Rudwi PradestaNoch keine Bewertungen
- Multiple Care Plan Factsheet 270314Dokument6 SeitenMultiple Care Plan Factsheet 270314Leonard YangNoch keine Bewertungen
- Form Self Assessment Diagnosa Non Spesialistik Kompetensi 4ADokument6 SeitenForm Self Assessment Diagnosa Non Spesialistik Kompetensi 4Asabita dwiratnaNoch keine Bewertungen
- Medical solutions, preparations and equipment listDokument6 SeitenMedical solutions, preparations and equipment listGheorghe PanasNoch keine Bewertungen
- Danger Signs in NewbornDokument8 SeitenDanger Signs in NewbornPrabhu MagudeeswaranNoch keine Bewertungen
- Data ResepDokument26 SeitenData ResepFACHRIZAL AMRIENoch keine Bewertungen
- Soap Hari 1 & 2 (19Dokument19 SeitenSoap Hari 1 & 2 (19Mitra Aditama AktifNoch keine Bewertungen
- What Is Viral Pneumonia?: 8th Leading Cause of Death Children and People Over 65Dokument10 SeitenWhat Is Viral Pneumonia?: 8th Leading Cause of Death Children and People Over 65Andeariesa DarmansiusNoch keine Bewertungen
- Journal CubDokument33 SeitenJournal CubHaritha K MuraleedharanNoch keine Bewertungen
- OMEPRAZOLEDokument5 SeitenOMEPRAZOLEElizabeth Ivory Chua100% (1)
- Clindamycin Drug StudyDokument3 SeitenClindamycin Drug StudygoyaNoch keine Bewertungen
- Preterm LaborDokument29 SeitenPreterm LaborBer AnneNoch keine Bewertungen
- Master DDD 2017Dokument904 SeitenMaster DDD 2017Ainul YuyunNoch keine Bewertungen
- LAPORAN MUTASI BHP LABORATORIUM BULAN JANUARI 2019Dokument32 SeitenLAPORAN MUTASI BHP LABORATORIUM BULAN JANUARI 2019tely rodjaNoch keine Bewertungen
- Peritonsillar Abscess (Quinsy)Dokument18 SeitenPeritonsillar Abscess (Quinsy)Michael AmandyNoch keine Bewertungen
- HyperthyroidismDokument11 SeitenHyperthyroidismKaraLyn HatcherNoch keine Bewertungen
- Cotrimoxazole SyDokument4 SeitenCotrimoxazole Syshanti apriyanthiNoch keine Bewertungen
- Major R Cance Er Miles Stones: Overvie EwDokument14 SeitenMajor R Cance Er Miles Stones: Overvie Ewtkobosz4877Noch keine Bewertungen
- COMMON OBSTETRIC MANAGEMENT GUIDELINESDokument7 SeitenCOMMON OBSTETRIC MANAGEMENT GUIDELINESaslanNoch keine Bewertungen
- Medicine 2019-2008 Regular-Supplementary Group Wise Question Papers WBUHS-1 PDFDokument24 SeitenMedicine 2019-2008 Regular-Supplementary Group Wise Question Papers WBUHS-1 PDFAditya Barman100% (1)
- CPG Uti PDFDokument7 SeitenCPG Uti PDFhellokathyyyyyyNoch keine Bewertungen
- Medication dosage and treatment options quizDokument2 SeitenMedication dosage and treatment options quizYanyan071680% (10)
- Amiodarone Increases Plasma Digoxin ConcentrationsDokument1 SeiteAmiodarone Increases Plasma Digoxin Concentrationseki_megaraniNoch keine Bewertungen
- Skripsi. Jurnal Untan - Ac.id Miopi PDFDokument20 SeitenSkripsi. Jurnal Untan - Ac.id Miopi PDFrifkaraihanaNoch keine Bewertungen
- Comprehensive ROS ReviewDokument13 SeitenComprehensive ROS ReviewDenz Marc AleaNoch keine Bewertungen