Das könnte Ihnen auch gefallen
- Primary and Secondary Survey-Dr. Joan Willy Ansar, Span - PPT NewDokument17 SeitenPrimary and Secondary Survey-Dr. Joan Willy Ansar, Span - PPT NewPrabu Tirta AjiNoch keine Bewertungen
- AAO Network CataractDokument53 SeitenAAO Network CataractsafasayedNoch keine Bewertungen
- Penetrating Keratoplasty StepsDokument57 SeitenPenetrating Keratoplasty StepsVishwajeetNoch keine Bewertungen
- Hordeolum - Background, Pathophysiology, EpidemiologyDokument6 SeitenHordeolum - Background, Pathophysiology, EpidemiologyKeren SingamNoch keine Bewertungen
- Hasil Tesis AdelaideDokument93 SeitenHasil Tesis AdelaideAndi Alfian Zainuddin100% (1)
- Glaucoma LectureDokument166 SeitenGlaucoma LectureSonali Gupta100% (1)
- Devgan. Phaco Fundamentals. BookDokument29 SeitenDevgan. Phaco Fundamentals. Bookjuanjorlopez100% (3)
- Cataract 20surgery 2029 05 2008 131224024457 Phpapp01Dokument61 SeitenCataract 20surgery 2029 05 2008 131224024457 Phpapp01Bboy ToonNoch keine Bewertungen
- Pars Plana VitrectomyDokument6 SeitenPars Plana VitrectomyAndreas OctavianoNoch keine Bewertungen
- Cataract SurgeryDokument2 SeitenCataract SurgeryndrabramsNoch keine Bewertungen
- Glaucoma GuidelinesDokument28 SeitenGlaucoma GuidelinesRina RostianaNoch keine Bewertungen
- CATARACTDokument25 SeitenCATARACTDea NabilaNoch keine Bewertungen
- Komplikasi Operasi KatarakDokument130 SeitenKomplikasi Operasi KatarakMauVeeNoch keine Bewertungen
- Cataract Classification 2003Dokument8 SeitenCataract Classification 2003Abdelrahman M. AlnweiriNoch keine Bewertungen
- Small Incision Cataract SurgeryDokument249 SeitenSmall Incision Cataract Surgeryirina100% (1)
- Managing Complications in Glaucoma SurgeryDokument121 SeitenManaging Complications in Glaucoma Surgeryshetya_8212Noch keine Bewertungen
- LEUKOKORIADokument3 SeitenLEUKOKORIAFahlevie EpinNoch keine Bewertungen
- Presentasi Kasus Glaukoma AkutDokument24 SeitenPresentasi Kasus Glaukoma AkutHendrawan Ariwibowo100% (1)
- Aao Bab 4Dokument3 SeitenAao Bab 4ria mutiaraNoch keine Bewertungen
- Subluksasi LensaDokument12 SeitenSubluksasi LensaDede GunawanNoch keine Bewertungen
- Limbal DermoidDokument4 SeitenLimbal DermoidPranjali ChhayaNoch keine Bewertungen
- Trauma MataDokument57 SeitenTrauma MataFatmala Umi MaisarahNoch keine Bewertungen
- Bullous Keratopathy PRDokument12 SeitenBullous Keratopathy PRshevinesaNoch keine Bewertungen
- RetinaDokument82 SeitenRetinafebienaNoch keine Bewertungen
- Posterior Capsular OpacityDokument3 SeitenPosterior Capsular OpacityRandy FerdianNoch keine Bewertungen
- RozerplastyDokument4 SeitenRozerplastyLutfi Aulia RahmanNoch keine Bewertungen
- 1 - Perbandingan Teknik Endoscopic Third VentriculostomyDokument10 Seiten1 - Perbandingan Teknik Endoscopic Third VentriculostomyKathryn TurnerNoch keine Bewertungen
- EviserasiDokument5 SeitenEviserasiristaniatauhidNoch keine Bewertungen
- Operasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarDokument10 SeitenOperasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarBlack Clover IdNoch keine Bewertungen
- Secondary Angle Closure GlaucomaDokument35 SeitenSecondary Angle Closure GlaucomaAndriati NadhilaNoch keine Bewertungen
- Acute Scrotum 231016 PDFDokument50 SeitenAcute Scrotum 231016 PDFDany Dias100% (1)
- Soal OFKOMDokument3 SeitenSoal OFKOMDian ArianiNoch keine Bewertungen
- Hifema: Rizky Amalia Palupi Bobi Ahmad Sahid LuthfiDokument21 SeitenHifema: Rizky Amalia Palupi Bobi Ahmad Sahid Luthfidr.Bobi Ahmad Sahid, S.KepNoch keine Bewertungen
- Seidel's TestDokument13 SeitenSeidel's TestFahcrezaNoch keine Bewertungen
- Correlation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliDokument3 SeitenCorrelation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliKarina NathaniaNoch keine Bewertungen
- Spesifikasi TEUFEL Cataract SetDokument1 SeiteSpesifikasi TEUFEL Cataract SetpatriceNoch keine Bewertungen
- De La Maza, Maite Sainz, MD, Phd. Scleritis. 2010. (Diakses Tanggal)Dokument1 SeiteDe La Maza, Maite Sainz, MD, Phd. Scleritis. 2010. (Diakses Tanggal)fa dliNoch keine Bewertungen
- 30secondary GlaucomasDokument19 Seiten30secondary GlaucomasShari' Si WahyuNoch keine Bewertungen
- Corne A: Dr. Yulia Fitriani, SPMDokument47 SeitenCorne A: Dr. Yulia Fitriani, SPMEdsel QasswaraNoch keine Bewertungen
- Hyphema 2Dokument7 SeitenHyphema 2heidyNoch keine Bewertungen
- RAPDDokument2 SeitenRAPDAlpascaFirdausNoch keine Bewertungen
- Taping OA Genu Dr. SIsca Susantio, Sp. KFRDokument11 SeitenTaping OA Genu Dr. SIsca Susantio, Sp. KFRDsk IndryNoch keine Bewertungen
- GonioskopiDokument40 SeitenGonioskopiRaissaNoch keine Bewertungen
- 13 - 266fourniers Gangrene PDFDokument5 Seiten13 - 266fourniers Gangrene PDFMochamad RizalNoch keine Bewertungen
- Pityriasis Rosea - Background, Pathophysiology, EtiologyDokument4 SeitenPityriasis Rosea - Background, Pathophysiology, EtiologysyahrulroziNoch keine Bewertungen
- 19 Rationale of Retinal Detachment ManagementDokument87 Seiten19 Rationale of Retinal Detachment ManagementvajasaNoch keine Bewertungen
- Jaundice: Slide 001Dokument91 SeitenJaundice: Slide 001mel_napsterNoch keine Bewertungen
- Diagram For Ophtal NoteDokument7 SeitenDiagram For Ophtal NoteSiam Weng LoongNoch keine Bewertungen
- Tinea UnguiumDokument8 SeitenTinea UnguiumwirdahajaNoch keine Bewertungen
- Cataract Surgery in Retina PatientsDokument21 SeitenCataract Surgery in Retina PatientsAnonymous 4OnqyBErNoch keine Bewertungen
- Short Case 1 PterygiumDokument15 SeitenShort Case 1 PterygiumAnmol KhadkaNoch keine Bewertungen
- 14th SOM LAMPUNG 2020 PROPOSALDokument23 Seiten14th SOM LAMPUNG 2020 PROPOSALnovitaNoch keine Bewertungen
- Anesthesia For Opthalmological SurgeriesDokument69 SeitenAnesthesia For Opthalmological SurgeriesRajesh MunigialNoch keine Bewertungen
- Laser Iridotomy and GlaucomaDokument2 SeitenLaser Iridotomy and Glaucomajo_jo_maniaNoch keine Bewertungen
- CP AmbliopiaDokument35 SeitenCP AmbliopiaNuruel SazaNoch keine Bewertungen
- Corneal Drawing and Other StructureDokument2 SeitenCorneal Drawing and Other StructureOden Mahyudin50% (2)
- Ophthalmology Card AnswersDokument29 SeitenOphthalmology Card AnswersRaihan MahmudNoch keine Bewertungen
- BCSC Reading Schedule 2020-2021Dokument13 SeitenBCSC Reading Schedule 2020-2021StefanieNoch keine Bewertungen
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaVon EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaNoch keine Bewertungen
- A Simple Guide to Ankle Dislocation, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Ankle Dislocation, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Peroperative Complications of Cataract Surgery: Jaidev Vishwa 3 Year Supplementary Roll No 11Dokument23 SeitenPeroperative Complications of Cataract Surgery: Jaidev Vishwa 3 Year Supplementary Roll No 11jaidev vishwaNoch keine Bewertungen
- Jurnal ReadingDokument4 SeitenJurnal ReadingArum DiannitasariNoch keine Bewertungen
- CV-30000-FortasE 8P 7Dokument8 SeitenCV-30000-FortasE 8P 7PAULO SOUZANoch keine Bewertungen
- Eye DisordersDokument14 SeitenEye DisordersAireen Grace GilosNoch keine Bewertungen
- Capsular Tension Rings:: Current Indications and OutcomesDokument12 SeitenCapsular Tension Rings:: Current Indications and OutcomesShahid ManzoorNoch keine Bewertungen
- Ophthalmology Card AnswersDokument29 SeitenOphthalmology Card AnswersRaihan MahmudNoch keine Bewertungen
- Maria Alexandra Preda: Curriculum VitaeDokument4 SeitenMaria Alexandra Preda: Curriculum VitaeVlad FărăuNoch keine Bewertungen
- Ophthalmology Instruments & LensDokument39 SeitenOphthalmology Instruments & LensShahbaz AAnsariNoch keine Bewertungen
- Phaco Cataract Surgery Package ChargesDokument1 SeitePhaco Cataract Surgery Package ChargesNeyaz HasnainNoch keine Bewertungen
- OphthBusinessApril 2010 PDFDokument27 SeitenOphthBusinessApril 2010 PDFDana Andreea PopescuNoch keine Bewertungen
- ICO Residency-Curriculum PDFDokument219 SeitenICO Residency-Curriculum PDFJujunNoch keine Bewertungen
- CGHS Rates 2014 - Nagpur1Dokument58 SeitenCGHS Rates 2014 - Nagpur1RajatNoch keine Bewertungen
- Peroperative Complications of Cataract Surgery: Jaidev Vishwa 3 Year Supplementary Roll No 11Dokument23 SeitenPeroperative Complications of Cataract Surgery: Jaidev Vishwa 3 Year Supplementary Roll No 11jaidev vishwaNoch keine Bewertungen
- Kanski - Chapter 9Dokument9 SeitenKanski - Chapter 9snylstlNoch keine Bewertungen
- MCQs For FRCOphth Part 2Dokument253 SeitenMCQs For FRCOphth Part 2Sherein HagrasNoch keine Bewertungen
- Medicsindex Egypt Member Profile DR Ahmad ElmassryDokument9 SeitenMedicsindex Egypt Member Profile DR Ahmad ElmassryMedicsindex Telepin Slidecase100% (15)
- PhacoemulsificationDokument22 SeitenPhacoemulsificationchQNoch keine Bewertungen
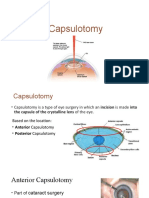
- CapsulotomyDokument15 SeitenCapsulotomyAdrian PearlNoch keine Bewertungen
- Endophthalmitis Harry Flynn MD OEDokument31 SeitenEndophthalmitis Harry Flynn MD OEMsai AhyarNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyDokument6 SeitenSenile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyadliahghaisaniNoch keine Bewertungen
- Cataract Surgery With Phaco & Femtophaco TechniqueDokument193 SeitenCataract Surgery With Phaco & Femtophaco TechniqueRajesh GuptaNoch keine Bewertungen
- Cataract Surgery After Vitrectomy - Phacovitrectomy - American Academy of OphthalmologyDokument5 SeitenCataract Surgery After Vitrectomy - Phacovitrectomy - American Academy of OphthalmologyAlejandro N. Fonseca GrandaNoch keine Bewertungen
- Yoga ResumeDokument4 SeitenYoga ResumeYoga SriNoch keine Bewertungen
- Katena Mejor CatalogDokument242 SeitenKatena Mejor Catalogibor747Noch keine Bewertungen
- Ilyas S, Yulianti SR. Ilmu Penyakit Mata. Edisi 5. Fakultas Kedokteran. Universitas Indonesia. 2014Dokument2 SeitenIlyas S, Yulianti SR. Ilmu Penyakit Mata. Edisi 5. Fakultas Kedokteran. Universitas Indonesia. 2014michelahengrawiNoch keine Bewertungen
- (Essentials in Ophthalmology) Ahmad A. Aref, Rohit Varma (Eds.) - Advanced Glaucoma Surgery-Springer International Publishing (2015)Dokument140 Seiten(Essentials in Ophthalmology) Ahmad A. Aref, Rohit Varma (Eds.) - Advanced Glaucoma Surgery-Springer International Publishing (2015)Inna Bujor100% (1)
- Kudakwashe Research Project Proposal 19 MayDokument14 SeitenKudakwashe Research Project Proposal 19 MayKudakwashe MagogoNoch keine Bewertungen
- Daftar PustakaDokument8 SeitenDaftar PustakaStefan SaerangNoch keine Bewertungen
- 2012 Katalyst Surgical Catalog PDFDokument69 Seiten2012 Katalyst Surgical Catalog PDFDien Doan QuangNoch keine Bewertungen