Das könnte Ihnen auch gefallen
- Helping Children and Adolescents with Chronic and Serious Medical Conditions: A Strengths-Based ApproachVon EverandHelping Children and Adolescents with Chronic and Serious Medical Conditions: A Strengths-Based ApproachNoch keine Bewertungen
- Child and Adolescent Psychiatry for PediatriciansVon EverandChild and Adolescent Psychiatry for PediatriciansNoch keine Bewertungen
- Conceptual Model of Mental Illness RecoveryDokument4 SeitenConceptual Model of Mental Illness RecoveryemaildegeorgeNoch keine Bewertungen
- 12 PDFDokument201 Seiten12 PDFaastha jainNoch keine Bewertungen
- Bipolar Disorder in Children and Adolescents An Update On DiagnosisDokument12 SeitenBipolar Disorder in Children and Adolescents An Update On DiagnosisLAURA FRITSCHE GARCIANoch keine Bewertungen
- Case Presentation PBL 12 Bipolar DisorderDokument65 SeitenCase Presentation PBL 12 Bipolar DisorderKim S GutierrezNoch keine Bewertungen
- Dependent Personality Disorder - A Review of Etiology and TreatmenDokument12 SeitenDependent Personality Disorder - A Review of Etiology and TreatmenTonia LoizidouNoch keine Bewertungen
- Childhood Disorders 1. Autism: Izzy WayDokument9 SeitenChildhood Disorders 1. Autism: Izzy WayKim GonzalesNoch keine Bewertungen
- PsychosisDokument32 SeitenPsychosisRamya Gopala KrishnanNoch keine Bewertungen
- DSM V Clinical Cases - Chapter 12 Sleep Wake DisordersDokument13 SeitenDSM V Clinical Cases - Chapter 12 Sleep Wake DisordersIzzyinOzzieNoch keine Bewertungen
- Very Early and Early Onset SchizophreniaDokument4 SeitenVery Early and Early Onset SchizophreniaahmadreyhaanNoch keine Bewertungen
- Comprehensive Case Conceptualization - FinalDokument29 SeitenComprehensive Case Conceptualization - Finalapi-708454518Noch keine Bewertungen
- Scales For ProdromeDokument15 SeitenScales For Prodromedrkadiyala2Noch keine Bewertungen
- Spencer Et Al-2021-Child and Adolescent Psychiatry and Mental HealthDokument12 SeitenSpencer Et Al-2021-Child and Adolescent Psychiatry and Mental HealthKJ HiramotoNoch keine Bewertungen
- Why Do LGBTQ Youths in America Feel The Need To Hide 1Dokument13 SeitenWhy Do LGBTQ Youths in America Feel The Need To Hide 1api-609315513Noch keine Bewertungen
- Fitzgerald - Child Psychoanalytic PsychotherapyDokument8 SeitenFitzgerald - Child Psychoanalytic PsychotherapyJulián Alberto Muñoz FigueroaNoch keine Bewertungen
- Aggression in Psychiatry Wards A Systematic ReviewDokument11 SeitenAggression in Psychiatry Wards A Systematic ReviewFernanda Vidal AndradeNoch keine Bewertungen
- 2 Bipolar DisorderDokument9 Seiten2 Bipolar DisorderJuan Carlos Veloso RetamalNoch keine Bewertungen
- Guide To Assessment Scales in Major Depressive DisorderDokument80 SeitenGuide To Assessment Scales in Major Depressive DisorderKartika AyuNoch keine Bewertungen
- Clinical Assessment and Management of Child and Adolescent Psychiatric EmergenciesDokument39 SeitenClinical Assessment and Management of Child and Adolescent Psychiatric EmergenciesRyan Lazatin100% (1)
- 2001 - Schizophrenia in Children and Adolescents - RemschmidtDokument322 Seiten2001 - Schizophrenia in Children and Adolescents - RemschmidtvdenkerNoch keine Bewertungen
- Literature ReviewDokument9 SeitenLiterature ReviewCarlee ChynowethNoch keine Bewertungen
- Malta Postgraduate Psychiatry ProgrammeDokument60 SeitenMalta Postgraduate Psychiatry Programmepsy6754100% (1)
- APSS (Attenuated Psychotic Symptoms Syndrome)Dokument40 SeitenAPSS (Attenuated Psychotic Symptoms Syndrome)drkadiyala2Noch keine Bewertungen
- Spiritual Care For A Terminally Ill PatientDokument4 SeitenSpiritual Care For A Terminally Ill PatientMohd Khairullah Mohd IdzharNoch keine Bewertungen
- Oxford Textbook of Old Age PsychiatryDokument7 SeitenOxford Textbook of Old Age PsychiatryCengizhan ErNoch keine Bewertungen
- Psychological Approaches To Bipolar Disorders: A Theoretical CritiqueDokument22 SeitenPsychological Approaches To Bipolar Disorders: A Theoretical CritiqueGary CadfaelNoch keine Bewertungen
- Rad Case Study Child-Based Research Review & ReflectionDokument17 SeitenRad Case Study Child-Based Research Review & Reflectionapi-282525755Noch keine Bewertungen
- Depression (Major Depressive Disorder) : Mental Health Notes™Dokument38 SeitenDepression (Major Depressive Disorder) : Mental Health Notes™Kyla GarciaNoch keine Bewertungen
- Annual Review of Addictions and Offender Counseling, Volume IV: Best PracticesVon EverandAnnual Review of Addictions and Offender Counseling, Volume IV: Best PracticesNoch keine Bewertungen
- MAKING SENSE OF PSYCHIATRY: An Insecure ProfessionDokument24 SeitenMAKING SENSE OF PSYCHIATRY: An Insecure ProfessionPaul Minot MDNoch keine Bewertungen
- Yossr Book Links CollectionDokument302 SeitenYossr Book Links CollectionHind Ben HadouNoch keine Bewertungen
- Schizotipy Review and Relationship With SchizophreniaDokument11 SeitenSchizotipy Review and Relationship With Schizophreniasofian2pNoch keine Bewertungen
- Neurocognitve DisordersDokument24 SeitenNeurocognitve Disordershassaan aliNoch keine Bewertungen
- Module 3 Biochemistry of The BrainDokument12 SeitenModule 3 Biochemistry of The BrainSakshi Jauhari100% (1)
- Obsessive-Compulsive Disorder - StatPearls - NCBI BookshelfDokument7 SeitenObsessive-Compulsive Disorder - StatPearls - NCBI BookshelfDhany karubuyNoch keine Bewertungen
- ICD 10 and DSM 5 Diffrence DDKFDDokument2 SeitenICD 10 and DSM 5 Diffrence DDKFDEmraan Malik100% (1)
- Review of The Worldwide Epidemiology of Eating DisordersDokument4 SeitenReview of The Worldwide Epidemiology of Eating DisordersInês RodriguesNoch keine Bewertungen
- PDF - How To Manage An Agitated Patient PDFDokument9 SeitenPDF - How To Manage An Agitated Patient PDFAlexandr SocrovisciucNoch keine Bewertungen
- Notes On PsychiatryDokument10 SeitenNotes On PsychiatryMark VillenaNoch keine Bewertungen
- MHA Ect GuidelinesDokument151 SeitenMHA Ect GuidelinesDian AfrisiaNoch keine Bewertungen
- Psychiatry Online - American Journal of Psychiatry - Psychiatric Disorders inDokument13 SeitenPsychiatry Online - American Journal of Psychiatry - Psychiatric Disorders inAnnemarie AppletonNoch keine Bewertungen
- Classification in PsychiatryDokument19 SeitenClassification in PsychiatrypaulraviNoch keine Bewertungen
- Lecture 9. Special Care - Terminal & Palliative CareDokument25 SeitenLecture 9. Special Care - Terminal & Palliative CareAnn Heerah100% (1)
- Bipolar DisorderDokument13 SeitenBipolar Disorderapi-3487528750% (1)
- This Case Is FictitiousDokument13 SeitenThis Case Is FictitiousJackeline Mendoza BurgaNoch keine Bewertungen
- Mental Health Information For Children: Child PsychiatryDokument9 SeitenMental Health Information For Children: Child Psychiatryedawood2100% (2)
- Treatment Resistent Depression ArticleDokument6 SeitenTreatment Resistent Depression Articlewaqas724Noch keine Bewertungen
- Parenting Stress, Child Adjustment, and Future Research QuestionsDokument19 SeitenParenting Stress, Child Adjustment, and Future Research QuestionsBianca SerafincianuNoch keine Bewertungen
- Psychiatric Emergencies in Children - FinalDokument89 SeitenPsychiatric Emergencies in Children - Finalslacker77725Noch keine Bewertungen
- G.berrios MentalDokument581 SeitenG.berrios MentalRicardo Branco Julião100% (1)
- (Hollon, 2010) - The Cognitive RevolutionDokument12 Seiten(Hollon, 2010) - The Cognitive RevolutionEileen GarcíaNoch keine Bewertungen
- NEW RESEARCH AntipshychoticDokument319 SeitenNEW RESEARCH AntipshychoticLaura BechtolsheimerNoch keine Bewertungen
- Mental health and HIV in IndiaDokument7 SeitenMental health and HIV in IndiaAyu RajikanNoch keine Bewertungen
- Mood DisordersDokument6 SeitenMood Disordersapi-217446206Noch keine Bewertungen
- 21.cpsy.034 Icd-10&dsm-5Dokument8 Seiten21.cpsy.034 Icd-10&dsm-5Victor YanafNoch keine Bewertungen
- Forensic Psychiatry Part1Dokument25 SeitenForensic Psychiatry Part1JasonNoch keine Bewertungen
- Marcadores Cerebrales y EsquizofreniaDokument6 SeitenMarcadores Cerebrales y EsquizofreniaDanitza YhovannaNoch keine Bewertungen
- Crisis PsicogenasDokument6 SeitenCrisis PsicogenasDanitza YhovannaNoch keine Bewertungen
- Consideraciones Psiquiatricas en Oncologia - R1 Dino PDFDokument16 SeitenConsideraciones Psiquiatricas en Oncologia - R1 Dino PDFDanitza YhovannaNoch keine Bewertungen
- Articulo. Exploring The Use of Chronic Opioid Therapy For Chronic PainDokument22 SeitenArticulo. Exploring The Use of Chronic Opioid Therapy For Chronic PainDanitza YhovannaNoch keine Bewertungen
- Entrevista Motivacional Sobre La Adherencia A La Medicación en EZQDokument10 SeitenEntrevista Motivacional Sobre La Adherencia A La Medicación en EZQDanitza YhovannaNoch keine Bewertungen
- Manejo de Agitacion en Esquizofrenia y T. BipolarDokument8 SeitenManejo de Agitacion en Esquizofrenia y T. BipolarDanitza YhovannaNoch keine Bewertungen
- Interacción Entre Psicosis de Los Padres y Riesgo de EsquizofreniaDokument9 SeitenInteracción Entre Psicosis de Los Padres y Riesgo de EsquizofreniaDanitza YhovannaNoch keine Bewertungen
- Articulo. Treatment of Bipolar Disorders During Pregnancy PDFDokument23 SeitenArticulo. Treatment of Bipolar Disorders During Pregnancy PDFDanitza YhovannaNoch keine Bewertungen
- Articulo. The Asthma Anxiety ConnectionDokument10 SeitenArticulo. The Asthma Anxiety ConnectionDanitza YhovannaNoch keine Bewertungen
- Articulo. Depression Induces Poor Prognosis AssociatesDokument12 SeitenArticulo. Depression Induces Poor Prognosis AssociatesDanitza YhovannaNoch keine Bewertungen
- Articulo. Suicidio y Conducta SuicidaDokument13 SeitenArticulo. Suicidio y Conducta SuicidaDanitza YhovannaNoch keine Bewertungen
- Articulo. Effect of Preoperative Pain and Depressive Symptoms On TheDokument6 SeitenArticulo. Effect of Preoperative Pain and Depressive Symptoms On TheDanitza YhovannaNoch keine Bewertungen
- Articulo. Drug-Induced ParkinsonismDokument10 SeitenArticulo. Drug-Induced ParkinsonismDanitza YhovannaNoch keine Bewertungen
- Acute Confusion in ElderlyDokument12 SeitenAcute Confusion in ElderlyhoneyworksNoch keine Bewertungen
- Articulo. Enfermedad Renal y Deterioro CognitivoDokument14 SeitenArticulo. Enfermedad Renal y Deterioro CognitivoDanitza YhovannaNoch keine Bewertungen
- Complicaciones y Mortalidad en Pacientes Con Ezq y DBTDokument11 SeitenComplicaciones y Mortalidad en Pacientes Con Ezq y DBTDanitza YhovannaNoch keine Bewertungen
- Articulo. Electrolyte Disorders and AgingDokument7 SeitenArticulo. Electrolyte Disorders and AgingDanitza YhovannaNoch keine Bewertungen
- Effect of Long-Term Supplementation With FolicDokument9 SeitenEffect of Long-Term Supplementation With FolicDanitza YhovannaNoch keine Bewertungen
- Antipsicoticos de Largo Plazo en Primer EpisodioDokument11 SeitenAntipsicoticos de Largo Plazo en Primer EpisodioDanitza YhovannaNoch keine Bewertungen
- Adherence To Antidepressant Therapy - R2 ALVARODokument5 SeitenAdherence To Antidepressant Therapy - R2 ALVARODanitza YhovannaNoch keine Bewertungen
- Mejora de Validez en Investig Del Tratamiento de ComorbilidadDokument11 SeitenMejora de Validez en Investig Del Tratamiento de ComorbilidadDanitza YhovannaNoch keine Bewertungen
- Desorden Bipolar y Diabetes MellitusDokument11 SeitenDesorden Bipolar y Diabetes MellitusDanitza YhovannaNoch keine Bewertungen
- Tratamiento de Psicosis DepositoDokument5 SeitenTratamiento de Psicosis DepositoDanitza YhovannaNoch keine Bewertungen
- Evaluacion de Afectacion Cognitiva Por ElectrterapiaDokument6 SeitenEvaluacion de Afectacion Cognitiva Por ElectrterapiaDanitza YhovannaNoch keine Bewertungen
- Interacciones Mal Adaptativos de Amigdala PrefrontalDokument20 SeitenInteracciones Mal Adaptativos de Amigdala PrefrontalDanitza YhovannaNoch keine Bewertungen
- Tratamiento Ketamina en Dolor y DepresionDokument7 SeitenTratamiento Ketamina en Dolor y DepresionDanitza YhovannaNoch keine Bewertungen
- Riesgos Perinatales e Infancia Como Indicacores Premorbidos de Psicosis - r1 KeylaDokument16 SeitenRiesgos Perinatales e Infancia Como Indicacores Premorbidos de Psicosis - r1 KeylaDanitza YhovannaNoch keine Bewertungen
- Articulo. A Meta-Analysis of The Relationship Between Antidepressant Use in Pregnancy and TheDokument6 SeitenArticulo. A Meta-Analysis of The Relationship Between Antidepressant Use in Pregnancy and TheDanitza YhovannaNoch keine Bewertungen
- Efecto Neuroprotector de LitioDokument17 SeitenEfecto Neuroprotector de LitioDanitza YhovannaNoch keine Bewertungen
- Articulo. A Meta-Analysis of Olanzapine For The Prevention of Chemotherapy-Induced Nausea and VomitingDokument6 SeitenArticulo. A Meta-Analysis of Olanzapine For The Prevention of Chemotherapy-Induced Nausea and VomitingDanitza YhovannaNoch keine Bewertungen
- Joyce Travelbee: Human-to-Human RelationshipDokument20 SeitenJoyce Travelbee: Human-to-Human RelationshipJamesBuensalidoDellavaNoch keine Bewertungen
- Murder Mystery LabDokument19 SeitenMurder Mystery Labapi-451038689Noch keine Bewertungen
- H&P Cardio-Pul-Abd Checklist 2006Dokument6 SeitenH&P Cardio-Pul-Abd Checklist 2006lindseyNoch keine Bewertungen
- Or-Indicator Measure Profile-Kpi-6.4 Day Surgery Conversion To AdmissionDokument2 SeitenOr-Indicator Measure Profile-Kpi-6.4 Day Surgery Conversion To Admissionangeli punoNoch keine Bewertungen
- Time, Final Rinse Protocol and EndodonticsDokument1 SeiteTime, Final Rinse Protocol and EndodonticsvaamdevaaNoch keine Bewertungen
- UNIT 5 Factors Affecting The Healthcare System PDFDokument6 SeitenUNIT 5 Factors Affecting The Healthcare System PDFDana kristenNoch keine Bewertungen
- What Do Language Disorders Reveal About Brain-Language Relationships? From Classic Models To Network ApproachesDokument14 SeitenWhat Do Language Disorders Reveal About Brain-Language Relationships? From Classic Models To Network ApproachesvalentinepoulainNoch keine Bewertungen
- SURGERY Lecture 2 - Liver & Gallbladder (Dr. Wenceslao)Dokument19 SeitenSURGERY Lecture 2 - Liver & Gallbladder (Dr. Wenceslao)Medisina101100% (1)
- Laporan - Pendahuluan PJK FixDokument8 SeitenLaporan - Pendahuluan PJK FixNndaydnaNoch keine Bewertungen
- NCP: Labor Stage 1 Latent PhaseDokument9 SeitenNCP: Labor Stage 1 Latent PhaseJavieNoch keine Bewertungen
- Elizabeth Resume 2Dokument3 SeitenElizabeth Resume 2api-252417118Noch keine Bewertungen
- Leadership Shadowing ExperienceDokument2 SeitenLeadership Shadowing Experienceapi-437270264Noch keine Bewertungen
- Pelvic Floor StretchesDokument4 SeitenPelvic Floor StretchesABUBAKARNoch keine Bewertungen
- Question Excerpt From 96Dokument5 SeitenQuestion Excerpt From 96Lorainne FernandezNoch keine Bewertungen
- What Is Stress? Definition of StressDokument4 SeitenWhat Is Stress? Definition of StressJananee RajagopalanNoch keine Bewertungen
- Ambu BagDokument29 SeitenAmbu BagJessa Borre100% (2)
- The Eight Components of A Balanced SmileDokument13 SeitenThe Eight Components of A Balanced SmileMeshari Al- NafisiNoch keine Bewertungen
- One Cancer Cure - March 2012Dokument52 SeitenOne Cancer Cure - March 2012ed_corcoran83% (6)
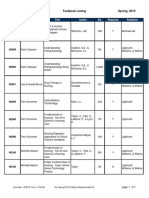
- BFLSON Course Textbook ListingDokument7 SeitenBFLSON Course Textbook ListingWina ViqaNoch keine Bewertungen
- 2015 Sigmoid DiverticulitisDokument11 Seiten2015 Sigmoid DiverticulitisDinNoch keine Bewertungen
- Final Health in The Hands of The PeopleDokument235 SeitenFinal Health in The Hands of The PeopleGodfrey Josef TorresNoch keine Bewertungen
- Jurnal Studi Kasus AskepDokument8 SeitenJurnal Studi Kasus Askepaji bayuNoch keine Bewertungen
- Unified Parkinson Disease Rating Scale - UPDRSDokument6 SeitenUnified Parkinson Disease Rating Scale - UPDRSJanakaVNoch keine Bewertungen
- Complaints Data Collection LetterDokument4 SeitenComplaints Data Collection LetterthrinathNoch keine Bewertungen
- ICU LogbookDokument37 SeitenICU Logbookrinus5100% (1)
- Head NursingDokument22 SeitenHead NursingGian Arlo Hilario CastroNoch keine Bewertungen
- Andre Hannah NursingresumeDokument1 SeiteAndre Hannah Nursingresumeapi-450112281Noch keine Bewertungen
- Apollo Institute Graduates Ready for Healthcare CareersDokument60 SeitenApollo Institute Graduates Ready for Healthcare CareersboggalaNoch keine Bewertungen
- Conventional Tic Failure and Re TreatmentDokument25 SeitenConventional Tic Failure and Re TreatmentBruno Miguel Teixeira QueridinhaNoch keine Bewertungen
- Association of Voiding Dysfunction With Functional ConstipationDokument3 SeitenAssociation of Voiding Dysfunction With Functional ConstipationSisca Dwi AgustinaNoch keine Bewertungen