Das könnte Ihnen auch gefallen
- Types of AnemiaDokument6 SeitenTypes of AnemiaSittieNoch keine Bewertungen
- Hematology SummaryDokument9 SeitenHematology SummaryJovielle Hayden100% (1)
- RBC Morphology and InclusionsDokument3 SeitenRBC Morphology and InclusionsDeomicah SolanoNoch keine Bewertungen
- Blood Functions and ComponentsDokument3 SeitenBlood Functions and ComponentshelloaNoch keine Bewertungen
- AnaemiaDokument4 SeitenAnaemiaRichardNoch keine Bewertungen
- NUTRITIONAL ANEMIA GUIDEDokument7 SeitenNUTRITIONAL ANEMIA GUIDEoktavianprNoch keine Bewertungen
- MED (App17) - Approach To AnaemiaDokument5 SeitenMED (App17) - Approach To AnaemiaFlora XuNoch keine Bewertungen
- Hematology Guide to Anemia Etiology, Signs & Symptoms, Tests, and TreatmentDokument6 SeitenHematology Guide to Anemia Etiology, Signs & Symptoms, Tests, and TreatmentIman Sama-aliNoch keine Bewertungen
- ANEMIAS (Sickle Cell Anemia With Pathophysiology)Dokument31 SeitenANEMIAS (Sickle Cell Anemia With Pathophysiology)mabec pagaduan70% (10)
- PediatricDokument192 SeitenPediatricbolt boltNoch keine Bewertungen
- Hematology: FANER, Ned Denebe LACANILAO, Sunshine NUCUM, Billie Kim PAGADUAN, Maribec PUA, MonalisaDokument31 SeitenHematology: FANER, Ned Denebe LACANILAO, Sunshine NUCUM, Billie Kim PAGADUAN, Maribec PUA, MonalisatzuquinoNoch keine Bewertungen
- Anemia in Children: Causes, Types and TreatmentDokument61 SeitenAnemia in Children: Causes, Types and TreatmentSamuel ManurungNoch keine Bewertungen
- Anemia 2024Dokument50 SeitenAnemia 2024b9p6vmfnc4Noch keine Bewertungen
- Red blood cells pathology: An overview of regenerative, degenerative, and abnormal formsDokument20 SeitenRed blood cells pathology: An overview of regenerative, degenerative, and abnormal formsArnettaNoch keine Bewertungen
- AnemiaDokument35 SeitenAnemiaNatnael ShifferawNoch keine Bewertungen
- By Dr. Manal Said: Physiology Lecturer, Ain Shams UniversityDokument26 SeitenBy Dr. Manal Said: Physiology Lecturer, Ain Shams Universityeman el saeedNoch keine Bewertungen
- RBC anomalies-ANEMIADokument19 SeitenRBC anomalies-ANEMIAJeremiahNoch keine Bewertungen
- Sickle Cell AnemiaDokument37 SeitenSickle Cell Anemiahazelposis75% (4)
- Hematology Anemia & Bleeding Zorko2015Dokument6 SeitenHematology Anemia & Bleeding Zorko2015Rishi Sharma100% (1)
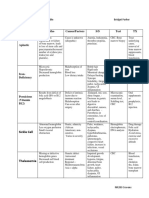
- Type Inheritance Pathogenesis Features Treatment: Iron Deficiency AnaemiaDokument4 SeitenType Inheritance Pathogenesis Features Treatment: Iron Deficiency AnaemiaNa NiNoch keine Bewertungen
- AnaemiaDokument25 SeitenAnaemiaIshali NuwanjiniNoch keine Bewertungen
- AnaemiaDokument83 SeitenAnaemiadoc19019696Noch keine Bewertungen
- Hematological Disorders: An Overview of Anemia, Sickle Cell Disease, and HemophiliaDokument4 SeitenHematological Disorders: An Overview of Anemia, Sickle Cell Disease, and Hemophilia3S - JOCSON, DENESE NICOLE LEE M.Noch keine Bewertungen
- Decreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisDokument8 SeitenDecreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisSamuel RothschildNoch keine Bewertungen
- Anemia - Aortic Stenosis B5Dokument8 SeitenAnemia - Aortic Stenosis B5Aila HinlogNoch keine Bewertungen
- Amboss Hemolytic AnemiaDokument16 SeitenAmboss Hemolytic AnemiaAhmed Ali100% (2)
- RBC DisordersDokument70 SeitenRBC DisordersNdor Baribolo100% (1)
- Anemia SDokument8 SeitenAnemia SCarlo SantosNoch keine Bewertungen
- Hematology and Oncology ' Hematology and Oncology ' Section IiiDokument20 SeitenHematology and Oncology ' Hematology and Oncology ' Section IiiLuis Jose VelazquezNoch keine Bewertungen
- Hema FinalsDokument12 SeitenHema FinalsHANA LUNARIANoch keine Bewertungen
- Lecture Lesson 9. Red Blood Cell DisordersDokument7 SeitenLecture Lesson 9. Red Blood Cell DisordersHANA LUNARIANoch keine Bewertungen
- Red Blood Cells PathologyDokument47 SeitenRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNoch keine Bewertungen
- HaematinicsDokument2 SeitenHaematinicsGerardLum100% (2)
- DR Irma - AnemiaDokument23 SeitenDR Irma - AnemiaWa JulianiNoch keine Bewertungen
- Anemia Table283Dokument2 SeitenAnemia Table283Bridget ParkerNoch keine Bewertungen
- Anemia - AmbossDokument10 SeitenAnemia - AmbossGuga XachidzeNoch keine Bewertungen
- 112 Lecture MidtermsDokument8 Seiten112 Lecture MidtermsRose Ann CammagayNoch keine Bewertungen
- 112 Lecture MidtermsDokument18 Seiten112 Lecture MidtermsRose Ann CammagayNoch keine Bewertungen
- Iron Defisience AnemiaDokument61 SeitenIron Defisience AnemiaYeni Jesika SilitongaNoch keine Bewertungen
- BloodDokument6 SeitenBloodBell GatesNoch keine Bewertungen
- ANEMIA TYPES AND CAUSESDokument8 SeitenANEMIA TYPES AND CAUSESsibanah menor100% (1)
- PathologyDokument30 SeitenPathologyPRAJWAL PES HDNoch keine Bewertungen
- Hoppt 20 SeptDokument19 SeitenHoppt 20 SeptmaisarahNoch keine Bewertungen
- Anemia DM-1 - REV.Dokument44 SeitenAnemia DM-1 - REV.abdulrahmanbelewa96Noch keine Bewertungen
- Decreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaDokument2 SeitenDecreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaIB leaksNoch keine Bewertungen
- AnaemiaDokument83 SeitenAnaemiaMohammad_Islam87100% (2)
- Anemia TutoringDokument28 SeitenAnemia TutoringngNoch keine Bewertungen
- RBC DisordersDokument27 SeitenRBC Disordersbpt2100% (1)
- Degenevie - HematologyDokument71 SeitenDegenevie - Hematologykkq7fhkwvkNoch keine Bewertungen
- Patho HematologyDokument39 SeitenPatho HematologyCastleKGNoch keine Bewertungen
- Hematologi ModulDokument67 SeitenHematologi ModulSyifa Mahmud Syukran Akbar100% (1)
- UntitledDokument3 SeitenUntitledSandeep m rNoch keine Bewertungen
- Hematology NotesDokument3 SeitenHematology NotesFarisa Jane BanggoNoch keine Bewertungen
- Approach To Diagnosis of Haemolytic AnaemiasDokument2 SeitenApproach To Diagnosis of Haemolytic AnaemiasGerardLumNoch keine Bewertungen
- Diseases in The Blood and Blood Forming OrgansDokument8 SeitenDiseases in The Blood and Blood Forming Organsbuenafe2000161Noch keine Bewertungen
- Fast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareVon EverandFast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareBewertung: 4 von 5 Sternen4/5 (1)
- BV, TV, Candidiasis Guide: Causes, Tests & TreatmentsDokument11 SeitenBV, TV, Candidiasis Guide: Causes, Tests & TreatmentsJason AnthonyNoch keine Bewertungen
- Medtech LawDokument16 SeitenMedtech LawClaudine David0% (1)
- Vitamins and Coenzymes: O O P O ODokument19 SeitenVitamins and Coenzymes: O O P O OKavita AtreNoch keine Bewertungen
- Protein Characterization Through Qualitative ReactionsDokument5 SeitenProtein Characterization Through Qualitative ReactionsJason AnthonyNoch keine Bewertungen
- Biochemistry MutationsDokument12 SeitenBiochemistry MutationsJason AnthonyNoch keine Bewertungen
- Bicohemistry Separation Techniques For ProteinsDokument2 SeitenBicohemistry Separation Techniques For ProteinsJason AnthonyNoch keine Bewertungen
- Phases in ReplicationDokument2 SeitenPhases in ReplicationJason AnthonyNoch keine Bewertungen
- Naming Nucleosides and NucleotidesDokument2 SeitenNaming Nucleosides and NucleotidesJason AnthonyNoch keine Bewertungen
- Amino Acid ReviewerDokument4 SeitenAmino Acid ReviewerJason AnthonyNoch keine Bewertungen
- Amino Acids I. Aliphatic: (Content From Maam Sarile's Lectures and Maam Esmalla's Notes)Dokument4 SeitenAmino Acids I. Aliphatic: (Content From Maam Sarile's Lectures and Maam Esmalla's Notes)Jason AnthonyNoch keine Bewertungen
- Practice QuestionsDokument130 SeitenPractice Questionsshirin kayNoch keine Bewertungen
- HEMA 1 ReviewerDokument14 SeitenHEMA 1 ReviewerAnonymous GT39EgNoch keine Bewertungen
- Hypoxia: Dr. Jyoti Prasad Deori Assistant Professor Dept of PhysiologyDokument35 SeitenHypoxia: Dr. Jyoti Prasad Deori Assistant Professor Dept of PhysiologyDorin PathakNoch keine Bewertungen
- Exp. On Hemoglobin Count - OliveDokument3 SeitenExp. On Hemoglobin Count - Olivejohn ferrerNoch keine Bewertungen
- Human Disorder & Gene TherapyDokument14 SeitenHuman Disorder & Gene Therapyulfh08152Noch keine Bewertungen
- Mapeh Health: Department of Educa I N Republi of The Philippines Health - Grade 7 Alternative Delivery ModeDokument17 SeitenMapeh Health: Department of Educa I N Republi of The Philippines Health - Grade 7 Alternative Delivery Modedarweng1988Noch keine Bewertungen
- Questions: A. Phenol B. Arsenic C. Mercury D. LeadDokument38 SeitenQuestions: A. Phenol B. Arsenic C. Mercury D. LeadJaved AkhtarNoch keine Bewertungen
- Anemia: Linda RottyDokument70 SeitenAnemia: Linda RottyKaren MogiNoch keine Bewertungen
- Pset 8 Solutions PDFDokument41 SeitenPset 8 Solutions PDFjoshua arnettNoch keine Bewertungen
- Nature's Healing Power Through FoodDokument565 SeitenNature's Healing Power Through FoodSangeetha Karthik100% (3)
- Drugs Acting On The Blood and The Blood-Forming Organs Pharmacology of Antianemic DrugsDokument6 SeitenDrugs Acting On The Blood and The Blood-Forming Organs Pharmacology of Antianemic DrugsanaNoch keine Bewertungen
- Study Guide CH 13 Nutr Care, AssessmentDokument3 SeitenStudy Guide CH 13 Nutr Care, AssessmentRoger manNoch keine Bewertungen
- Eng 2007 MedDokument42 SeitenEng 2007 MedLucia BogNoch keine Bewertungen
- Blood Cells Morphology Clinical Relevance 2nd EditionDokument42 SeitenBlood Cells Morphology Clinical Relevance 2nd Editionedson floresNoch keine Bewertungen
- Oral Manifestations of Systemic DiseasesDokument18 SeitenOral Manifestations of Systemic DiseasesYashpreetsingh BhatiaNoch keine Bewertungen
- Solomon B12 2006Dokument18 SeitenSolomon B12 2006Erwin K EdisonNoch keine Bewertungen
- Oman Pharmacist Licensing Exam McqsDokument186 SeitenOman Pharmacist Licensing Exam McqsMuhammad Amin100% (5)
- The Silverlight HeirDokument190 SeitenThe Silverlight HeirDominique DestréeNoch keine Bewertungen
- Quiz Questions On AnemiaDokument2 SeitenQuiz Questions On AnemiaSlooma100% (1)
- MRCP Syllabus-1Dokument19 SeitenMRCP Syllabus-1Medico HubNoch keine Bewertungen
- Interpretation of Peripheral SmearDokument34 SeitenInterpretation of Peripheral Smearswathi bs100% (1)
- Mix Questions PDFDokument40 SeitenMix Questions PDFZazo RawashdehNoch keine Bewertungen
- MCQ On Disorder of RBCS: Group (4) PresentsDokument6 SeitenMCQ On Disorder of RBCS: Group (4) PresentsIrekton GGNoch keine Bewertungen
- Rang and Dale's 14 - 22 - 25Dokument7 SeitenRang and Dale's 14 - 22 - 25jeskevandiemenNoch keine Bewertungen
- May 2011 TUS Exam - Clinical Sciences - TUS QuestionsDokument31 SeitenMay 2011 TUS Exam - Clinical Sciences - TUS QuestionsMohamedNoch keine Bewertungen
- Anemia in PregnancyDokument212 SeitenAnemia in Pregnancysalah subbah100% (1)
- Hematology Multiple Choice Questions Guide StudentsDokument5 SeitenHematology Multiple Choice Questions Guide StudentsMarie LlanesNoch keine Bewertungen
- Internal Medicine Highlights by Conrad Fischer (2008) PDFDokument34 SeitenInternal Medicine Highlights by Conrad Fischer (2008) PDFLi SacNoch keine Bewertungen
- Blood MCQDokument10 SeitenBlood MCQTennyson MachiwenyikaNoch keine Bewertungen
- Anemia Overview: The Third Hospital of Sun Yat-Sen UniversityDokument77 SeitenAnemia Overview: The Third Hospital of Sun Yat-Sen UniversityMazlina MaidinNoch keine Bewertungen