Sanchez Hernandez et al.
, J Diabetes Metab 2015, 6:3
Diabetes & Metabolism http://dx.doi.org/10.4172/2155-6156.1000505
Research Article Open Access
EZSCAN as a Screening Tool for Prediabetes and Diabetes in a Large
Mexican Population
Sanchez Hernandez OE1, Papacostas-Quintanilla H1, Vilier A2, Calvet JH2, Jimnez Osorio A1, Snchez Trampe BI1, Musalem Younes C1 and
Rodriguez-Arellano ME1*
1
Hospital Regional Lic. Adolfo Lpez Mateos, Institute for Social Security and Services for State Workers (ISSSTE), Mexico City, Mexico
2
Impeto Medical, Paris, France
Abstract
Objective: Autonomic neuropathy especially small C-Fibers innervating sweat glands is common in diabetes
and occurs in pre-diabetes. EZSCAN, a new and non-invasive device that precisely assesses sudomotor function
was evaluated as a screening tool for pre-diabetes and diabetes in a large Mexican population.
Methods: The study was performed in Hospital Regional Lic. Adolfo Lopez Mateos ISSSTE center. Subjects
were classified as pre-diabetic or diabetic according to ADA criteria for fasting plasma glucose (FPG) and HbA1C.
EZSCAN test was performed and subjects were classified as no risk, moderate risk or high risk and its performance
as a screening tool was assessed through ROC curve analysis.
Results: Among the 1414 subjects involved in the study 357 had pre-diabetes and 64 had diabetes according
to FPG confirmed by HbA1C for 52 of them. Area under the Curve for EZSCAN to detect pre-diabetes or diabetes
using FPG as reference were 0.65 and 0.73 respectively. Using 27 and 34 as threshold values for EZSCAN risk
score for detection of pre-diabetes and diabetes sensitivity was 69% and 73%, specificity 56% and 70% and negative
predictive value 82% and 98% respectively. The Odds Ratio (OR) for a patient classified as moderate risk with
EZSCAN test was 2.06 (1.59-2.67) to have pre-diabetes and 15.8 (3.8-65.5) to have diabetes as compared to a
subject with no risk. The OR was 4.32 (2.49-7.50) for pre-diabetes and 18.3 (3.3-102.5) for diabetes for a subject
with high risk as compared to a subject with no risk.
No adverse events during and after measurement with EZSCAN were reported.
Conclusion: EZSCAN allowing quick and quantitative assessment of sudomotor function could be used as an
early screening tool for pre-diabetes and diabetes in a large population before performance of more sophisticated
and specific, but time-consuming and expensive tests.
Keywords: Sudomotor function; Peripheral neuropathy; prevention on sweat chloride concentrations has been shown to detect sudomotor
dysfunction in people with diabetes or pre-diabetes when compared to
Introduction controls [10-14].
Type 2 diabetes is now recognized as an immense and growing The aim of this study was to evaluate EZSCAN as a screening tool
public health challenge worldwide affecting about 382 million adults for pre-diabetes and diabetes on a large Mexican population.
in 2014 and predicted to rise to 592 million by 2035 [1]. In Mexico,
the prevalence of pre-diabetes and diabetes were 10.7% and 12.7%, Materials and Methods
respectively in 2006 with an economic burden of more than US$750 The individuals invited to participate in the study were all recruited
million [2]. Early diagnosis of pre-diabetes and diabetes can result in in the Clinic Automated Detection and Diagnosis of the Institute for
appropriate interventions which can reduce the incidence of negative Social Security and Services for State Workers-ISSSTE (CLIDDA).
complications including myocardial infarction, stroke, retinopathy, After signing the informed consent a blood sample was taken and a test
nephropathy and neuropathy [3]. Therefore, it is of paramount with the ESZCAN was performed. Individuals over 18 years old of both
importance to adopt simple and inexpensive methods in screening sexes, apparently healthy, who attended a full check up at CLIDDA were
for individuals with high risk of pre-diabetes or diabetes. Autonomic
neuropathy is common in diabetes populations with potential
dysfunctions of cardiovascular, gastrointestinal, genitourinary systems
*Corresponding author: Rodriguez-Arellano Martha Eunice, Research
and sudomotor or ocular functions [4,5]. In addition, recent studies Department, Hospital Regional Lic., Adolfo Lpez Mateos, Av. Universidad
have shown that individuals with oral glucose intolerance can also 1321 Col. Florida, C.P. 01030, USA, Tel: 5253222300 (89203); E-mail:
develop autonomic neuropathy [6-8]. Sudomotor function disturbance marthaeunicer@yahoo.com.mx
is considered one of the initial components of autonomic neuropathy, Received January 09, 2015; Accepted February 28, 2015; Published March 05,
and its assessment may contribute to the detection of autonomic 2015
dysfunction in diabetics; in fact, the American Diabetes Association Citation: Sanchez Hernandez OE, Papacostas-Quintanilla H, Vilier A, Calvet JH,
suggests that sudomotor function assessing small fiber status should Jimnez Osorio A, et al. (2015) EZSCAN as a Screening Tool for Prediabetes
and Diabetes in a Large Mexican Population. J Diabetes Metab 6: 505.
be included in the diagnostic tests for the detection of neuropathies
doi:10.4172/2155-6156.1000505
in diabetes [5]. However lack of a simple and quick method has not
allowed widespread use of sudomotor function testing as a screening Copyright: 2015 Sanchez Hernandez OE, et al. This is an open-access article
distributed under the terms of the Creative Commons Attribution License, which
tool for diabetic neuropathies [9]. EZSCAN, a new device recently permits unrestricted use, distribution, and reproduction in any medium, provided
developed to allow a precise evaluation of sweat gland function based the original author and source are credited.
J Diabetes Metab Volume 6 Issue 3 1000505
ISSN: 2155-6156 JDM, an open access journal
Citation: Sanchez Hernandez OE, Papacostas-Quintanilla H, Vilier A, Calvet JH, Jimnez Osorio A, et al. (2015) EZSCAN as a Screening Tool for
Prediabetes and Diabetes in a Large Mexican Population. J Diabetes Metab 6: 505. doi:10.4172/2155-6156.1000505
Page 2 of 4
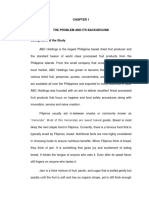
included. Individuals with a diagnosis of diabetes, chronic degenerative FPG as reference is displayed in Figure 2. AUC for HbA1C were 0.68
diseases, cancer, pregnant women and individuals with amputations for pre-diabetes and 0.92 for diabetes. Using 27 as a threshold value
were excluded. The protocol was approved by the committee of for EZSCAN score for detection of pre-diabetes (optimal according
research and research ethics committee for the Hospital Regional Lic. to Youden index), sensitivity was 69%, specificity 56% and negative
Adolfo Lopez Mateos with registration number 226.2013. predictive value 82%. Using 34 as threshold value for EZSCAN score for
detection of diabetes (optimal according to Youden index), sensitivity
Laboratory measurements was 73%, specificity 70% and negative predictive value 98 %. Among
Fasting plasma glucose (FPG) was measured using the glucose the 52 diabetic patients diagnosed through FPG and HbA1C only 2
oxidase method on an autoanalyser (Miura 200). Triglycerides (TG), had normal EZSCAN (no risk, 25). The OR for a patient classified as
and high-density lipoprotein cholesterol (HDL-C) were measured
using chemiluminescence methods on the autoanalyser (Miura 200).
The HbA1c level was measured by Immuno-turbidimetric Test Particle
Enhanced (Fully-automated Clinical Chemistry Analyzer Miura 200,
logotech-ise)
Prediabetes and diabetes were defined by FPG according to ADA
criteria (FPG between 100 and 125 mg/dL for prediabetes and 126
mg/dL for diabetes) [15].
Measurement of sweat function
EZSCAN is a patented device designed to perform a precise
evaluation of sweat gland function based on an electrochemical
reaction between sweat chloride and stainless-steel electrodes on which
a low Direct Current (DC) is applied and has been described previously
[16-19]. Its a dynamic method based on stimulation of sweat glands
by the low-level voltage, allowing evidence of sweat dysfunction not
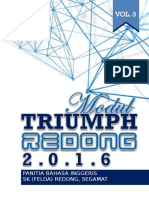
detectable under physiological conditions. The device consists of
two sets of electrodes for the feet and hands which are connected to
a computer for recording and data management (Figure 1). This is a
non-invasive test lasting approximately two minutes, during which
four combinations of 15 different low DC voltages are applied. No
subject preparation such as fasting is required for this test. The subject Figure 1: EZSCAN device with hand and foot electrodes. On the screen is
places their dry, clean palms of the hands and soles of the feet on the displayed a typical presentation of results after the test for a subject with
moderate risk.
electrodes. The device measures the Electrochemical Skin Conductance
(ESC) of the hands and feet (right and left sides) using the ratio of
the current measured over the constant power applied, expressed in
microSiemens (S). A risk score for prediabetes or diabetes is calculated
1.0
from these conductances and additional biometric data (age and BMI):
no risk ( 25), moderate risk (25-50) and high risk scores (>50). These
threshold values were issued from previous clinical studies. To improve
understanding of the results by the patient a color code for each risk
0.8
category is used (green for no risk, yellow for moderate risk and orange
for high risk).
0.6
Statistical analyses
Sensitivity
Results for quantitative variables are shown as means SD.
Quantitative variables were globally compared using ANOVA analysis.
0.4
As a rule, a p-value <0.05 was regarded as statistically significant.
EZSCAN performance was assessed using Receiver Operating Curve
(ROC) Analysis with calculation of the Area Under the Curve (AUC).
Odds ratios were calculated using logistic regression adjusted for
0.2
gender. The data management and statistical analysis were done using
SAS version 9.4 and R version 2.13.1 [20].
0.0
Results
0.0 0.2 0.4 0.6 0.8 1.0
Among the 1414 subjects involved in the study 357 had prediabetes
1-Specificity
and 64 had diabetes (among them 52 were confirmed by HbA1C
6.5%). Demographic data of the population are displayed in the Figure 2: Diagnostic performance of EZSCAN by receiving-operating
charactersitics (ROC) curve analysis for pre-diabetes (solid line) and diabetes
table. EZSCAN score values were higher in subjects with prediabetes (dotted line) using fasting plasma glucose threshold values as a gold-
and diabetes as compared to subjects with normal glucose tolerance. standard. Area under the curve are 0.65 for pre-diabetes 0.74 for diabetes.
Performance of EZSCAN to detect pre-diabetes and diabetes using
J Diabetes Metab Volume 6 Issue 3 1000505
ISSN: 2155-6156 JDM, an open access journal
Citation: Sanchez Hernandez OE, Papacostas-Quintanilla H, Vilier A, Calvet JH, Jimnez Osorio A, et al. (2015) EZSCAN as a Screening Tool for
Prediabetes and Diabetes in a Large Mexican Population. J Diabetes Metab 6: 505. doi:10.4172/2155-6156.1000505
Page 3 of 4
moderate risk with EZSCAN test as compared to a subject with no risk most successful approaches have been risk scores such as FINDRISC.
was 2.06 (1.59-2.67) to have pre-diabetes and 15.8 (3.8-65.5) to have A sensitivity rate of 6784% and specificity rate of 6167% for IGM
diabetes. The OR for a patient classified as high risk was 4.32 (2.49- have been reported from several studies [22,23]. Risk questionnaires
7.50) for pre-diabetes and 18.3 (3.3-102.5) for diabetes as compared to are non-invasive, technically simple, and low cost with reasonable
a subject with no risk according to EZSCAN test (Table 1). sensitivity and specificity; however, questions in a questionnaire can
sometimes be interpreted incorrectly if researchers are not available
No adverse event or discomfort during and after measurement
with EZSCAN was reported by any subject involved in the study. to clarify those questions, and the result of a questionnaire may also
be at risk of response bias. Furthermore, questionnaires often take
Discussion a considerable amount of time to complete and score. In comparison,
the non-invasive EZSCAN is an objective test requiring no input from
This study evidenced that the EZSCAN negative predictive values the subjects or operator, and the test takes only a couple of minutes to
for detection of pre-diabetes and diabetes were 82 and 98% respectively.
complete and provides immediate results with comparable sensitivity
Similar studies have been performed in countries with a and specificity. The other approach is FPG; however it requires
high prevalence of diabetes requiring a simple, quick and non- individuals to fast and has low sensitivity [24].
invasive method for screening of pre-diabetes and diabetes on large
EZSCAN was well accepted by the patients, in accordance with
populations. In a study performed in China on more than 5800 subjects
previous study populations [13]. As results are quantitative and
with a prevalence of pre-diabetes and diabetes of 21.9% and 17.5%
easy to understand they could also be used as a motivational tool for
respectively, Zhi Yang et al. showed that the optimal cut-off value for
lifestyle improvement. An exercise study in Finland of individuals at
detection of pre-diabetes and diabetes was 30% for EZSCAN risk score
[11]. Sensitivity was 73% for pre-diabetes and 81% for diabetes with cardiometabolic risk showed that subjects with higher weekly activity
specificities of 46 and 43% respectively. In another study performed - i.e. with a greater improvement in lifestyle - experienced a greater
in 876 subjects including 47% with impaired glucose metabolism the decrease in EZSCAN risk score after 12 months [25]. The results of
AUC of EZSCAN for detecting Impaired Glucose Metabolism (IGM) this last study were in line with small fiber recovery observed through
was 0.79 and with a cut-off of 40% EZSCAN score had a sensitivity of skin biopsy performed in patients involved in a lifestyle improvement
80%, a specificity of 72% and a negative predictive value of 87% for program [26]. In this way EZSCAN would be preferable for the follow-
the detection of IGM [10]. These two studies are in accordance with a up of a patient to questionnaires that do not take into account rapid
previous study performed in India. Ramachandran et al. evidenced that changes in lifestyle.
EZSCAN had a sensitivity of 75% to detect diabetes and 70% to detect One important limit of our study is that FPG was used as
pre-diabetes in patients diagnosed through an oral glucose tolerance reference. Oral glucose tolerance test (OGTT) would have been more
test [12]. suitable but could not be performed on such a large scale. The low
According to the results observed in this study, the performances percentage of diabetics in our population (around 4%) as compared to
of EZSCAN and HbA1C to detect pre-diabetes seem comparable while a percentage of 15-16% in the Mexican population could be explained
HbA1C has a higher capacity to detect diabetes. Based on this and on by the recruitment in a centre where patients have good follow-up. It
the low number of false negatives for diabetes (2 out of 52 diagnosed by underlines the importance of prevention.
FPG and confirmed by HbA1C), EZSCAN a quick, non-invasive and
This study shows that EZSCANa simple, non-invasive, quick and
easy to perform test could be suggested as a first screening test for
quantitative methodcould be used as a screening test for prediabetes
metabolic diseases in large populations. HbA1C is invasive, and requires
or diabetes before more specific, specialized, and time-consuming
time and cost to obtain the results; it would be performed only in
tests such as 2-hour OGTT or HbA1C. This will allow earlier detection
subjects with moderate or high risk according to EZSCAN test results.
of populations with high risk of developing or presenting diabetes,
This strategy would dramatically reduce costs avoiding performance of
numerous useless HbA1C tests whose individual cost is around $20 US. allowing implementation of preventive measures in this population.
There have been numerous attempts over the past 30 years to develop Acknowledgements
non-invasive methods to measure glucose or to use questionnaires/ We thank the Clinic detection and advanced diagnostic facilities for the
scores based on anthropometric data or other parameters for pre- recruitment of the sample used in this study.
diabetes/diabetes risk assessment as a first diagnostic step [21]. The
References
Whole population 1. International Diabetes Federation (2014) Diabetes Atlas (6thedtn). International
Diabetes Federation, Brussels.
(n=1414)
Age (yrs) 44.7 6.8 2. Arredondo A, De Icaza E (2011) [The cost of diabetes in Latin America:
Male, n(%) 702 (49.6) evidence from Mexico]. Value Health 14: S85-88.
EZSCAN risk score (%) 29.8 10.7 3. Fowler MJ (2008) Microvascular and macrovascular complications of diabetes.
BMI (kg/m) 28.6 4.5 Clinical diabetes 26: 77-82.
Waist circumference (cm) 95.5 11.0 4. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, et al. (2010) Diabetic
Hips circumference (cm) 103.5 10.1 neuropathies: update on definition, diagnostic criteria, estimation of severity
and treatments. Diabetes Care 33: 2285-2293.
Fasting plasma glucose (mg/dl) 98.3 25.6
HDL (mg/dl) 45.4 12.1 5. Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M (2003) The
spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology
Triglycerides (mg/dl) 169.4 101.8
60: 108-111.
HbA1C (%) 6.2 1.1
6. Kannan MA, Sarva S, Kandadai RM, Paturi VR, Jabeen SA, et al. (2014)
Data are Mean SD
Prevalence of neuropathy in patients with impaired glucose tolerance using
Table 1: Characteristics of the study population (n=1414). various electrophysiological tests. Neurol India 62: 656-661.
J Diabetes Metab Volume 6 Issue 3 1000505
ISSN: 2155-6156 JDM, an open access journal
Citation: Sanchez Hernandez OE, Papacostas-Quintanilla H, Vilier A, Calvet JH, Jimnez Osorio A, et al. (2015) EZSCAN as a Screening Tool for
Prediabetes and Diabetes in a Large Mexican Population. J Diabetes Metab 6: 505. doi:10.4172/2155-6156.1000505
Page 4 of 4
7. Ince H, Tademir HA, Aydin M, Ozyrek H, Tilki HE (2014) Evaluation of Nerve 18. Casellini CM, Parson HK, Richardson MS, Nevoret ML, Vinik AI (2013)
Conduction Studies in Obese Children With Insulin Resistance or Impaired Sudoscan, a noninvasive tool for detecting diabetic small fiber neuropathy and
Glucose Tolerance. J Child Neurol. autonomic dysfunction. Diabetes Technol Ther 15: 948-953.
8. Smith AG, Singleton JR (2008) Impaired glucose tolerance and neuropathy. 19. Eranki VG, Santosh R, Rajitha K, Pillai A, Sowmya P, et al. (2013) Sudomotor
Neurologist 14: 23-29. function assessment as a screening tool for microvascular complications in
type 2 diabetes. Diabetes Res Clin Pract 101: e11-13.
9. Low PA1 (2004) Evaluation of sudomotor function. Clin Neurophysiol 115:
1506-1513. 20. Dighe M, Bae U, Richardson ML, Dubinsky TJ, Minoshima S, et al. (2008)
Differential diagnosis of thyroid nodules with US elastography using carotid
10. Chen L, Chen X, Ding R, Shi Q Jr, Hu D (2013) Evaluation of EZSCAN as a artery pulsation. Radiology 248: 662-669.
screening tool for impaired glucose metabolism. Diabetes Res Clin Pract 100:
210-214. 21. Schwarz PE, Li J, Lindstrom J, Tuomilehto J (2009) Tools for predicting the risk
of type 2 diabetes in daily practice. Horm Metab Res 41: 86-97.
11. Yang Z, Xu B, Lu J, Tian X, Li M, et al. (2013) Autonomic test by EZSCAN in the
screening for prediabetes and diabetes. PLoS One 8: e56480. 22. Tankova T, Chakarova N, Atanassova I, Dakovska L (2011) Evaluation of the
Finnish Diabetes Risk Score as a screening tool for impaired fasting glucose,
12. Ramachandran A, Moses A, Shetty S, Thirupurasundari CJ, Seeli AC, et al. impaired glucose tolerance and undetected diabetes. Diabetes Res Clin Pract
(2010) A new non-invasive technology to screen for dysglycaemia including 92: 46-52.
diabetes. Diabetes Res Clin Pract 88: 302-306.
23. Makrilakis K, Liatis S, Grammatikou S, Perrea D, Stathi C, et al. (2011)
13. Schwarz P, Brunswick P, Calvet JH (2010) EZSCAN a new tool to detect Validation of the Finnish diabetes risk score (FINDRISC) questionnaire for
diabetes risk. British Journal of Diabetes and Vascular diseases 11: 204-209. screening for undiagnosed type 2 diabetes, dysglycaemia and the metabolic
14. Sheng CS, Zeng WF, Huang QF, Deslypere JP, Li Y, et al. (2011) Accuracy of syndrome in Greece. Diabetes Metab 37: 144-151.
a Novel Non-Invasive technology based EZSCAN system for the diagnosis of 24. Engelgau MM, Narayan KM, Herman WH (2000) Screening for type 2 diabetes.
diabetes mellitus in Chinese. Diabetol Metab Syndr 3: 36. Diabetes Care 23: 1563-1580.
15. American Diabetes Association (2010) Diagnosis and classification of diabetes 25. Raisanen A, Eklund J, Calvet JH, Tuomilehto J (2014) Sudomotor Function
mellitus. Diabetes Care 34: S62-69. as a Tool for Cardiorespiratory Fitness Level Evaluation: Comparison with
16. Smith AG, Lessard M, Reyna S, Doudova M, Singleton JR2 (2014) The Maximal Exercise Capacity. Int. J. Environ. Res. Public Health 11: 5839-5848.
diagnostic utility of Sudoscan for distal symmetric peripheral neuropathy. J 26. Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, et al. (2006) Lifestyle
Diabetes Complications 28: 511-516. intervention for pre-diabetic neuropathy. Diabetes Care 29: 1294-1299.
17. Freedman BI, Bowden DW, Smith SC, Xu J, Divers J4 (2014) Relationships
between electrochemical skin conductance and kidney disease in Type 2
diabetes. J Diabetes Complications 28: 56-60.
Submit your next manuscript and get advantages of OMICS
Group submissions
Unique features:
User friendly/feasible website-translation of your paper to 50 worlds leading languages
Audio Version of published paper
Digital articles to share and explore
Special features:
400 Open Access Journals
30,000 editorial team
21 days rapid review process
Quality and quick editorial, review and publication processing
Indexing at PubMed (partial), Scopus, EBSCO, Index Copernicus and Google Scholar etc
Citation: Sanchez Hernandez OE, Papacostas-Quintanilla H, Vilier A, Sharing Option: Social Networking Enabled
Calvet JH, Jimnez Osorio A, et al. (2015) EZSCAN as a Screening Tool for Authors, Reviewers and Editors rewarded with online Scientific Credits
Prediabetes and Diabetes in a Large Mexican Population. J Diabetes Metab 6: Better discount for your subsequent articles
505. doi:10.4172/2155-6156.1000505 Submit your manuscript at: www.editorialmanager.com/acrgroup
J Diabetes Metab Volume 6 Issue 3 1000505
ISSN: 2155-6156 JDM, an open access journal
Das könnte Ihnen auch gefallen
- tmp3CAB TMPDokument16 Seitentmp3CAB TMPFrontiersNoch keine Bewertungen
- tmpCE8C TMPDokument19 SeitentmpCE8C TMPFrontiersNoch keine Bewertungen
- tmpFFE0 TMPDokument6 SeitentmpFFE0 TMPFrontiersNoch keine Bewertungen
- tmpE7E9 TMPDokument14 SeitentmpE7E9 TMPFrontiersNoch keine Bewertungen
- tmp6F0E TMPDokument12 Seitentmp6F0E TMPFrontiersNoch keine Bewertungen
- tmpE3C0 TMPDokument17 SeitentmpE3C0 TMPFrontiersNoch keine Bewertungen
- tmpF178 TMPDokument15 SeitentmpF178 TMPFrontiersNoch keine Bewertungen
- tmp80F6 TMPDokument24 Seitentmp80F6 TMPFrontiersNoch keine Bewertungen
- tmpEFCC TMPDokument6 SeitentmpEFCC TMPFrontiersNoch keine Bewertungen
- Tmp1a96 TMPDokument80 SeitenTmp1a96 TMPFrontiersNoch keine Bewertungen
- tmpF3B5 TMPDokument15 SeitentmpF3B5 TMPFrontiersNoch keine Bewertungen
- Tmpa077 TMPDokument15 SeitenTmpa077 TMPFrontiersNoch keine Bewertungen
- tmp72FE TMPDokument8 Seitentmp72FE TMPFrontiersNoch keine Bewertungen
- tmpF407 TMPDokument17 SeitentmpF407 TMPFrontiersNoch keine Bewertungen
- tmpC0A TMPDokument9 SeitentmpC0A TMPFrontiersNoch keine Bewertungen
- tmp60EF TMPDokument20 Seitentmp60EF TMPFrontiersNoch keine Bewertungen
- tmp8B94 TMPDokument9 Seitentmp8B94 TMPFrontiersNoch keine Bewertungen
- tmp6382 TMPDokument8 Seitentmp6382 TMPFrontiersNoch keine Bewertungen
- tmp998 TMPDokument9 Seitentmp998 TMPFrontiersNoch keine Bewertungen
- tmp4B57 TMPDokument9 Seitentmp4B57 TMPFrontiersNoch keine Bewertungen
- tmp9D75 TMPDokument9 Seitentmp9D75 TMPFrontiersNoch keine Bewertungen
- tmp37B8 TMPDokument9 Seitentmp37B8 TMPFrontiersNoch keine Bewertungen
- tmpC30A TMPDokument10 SeitentmpC30A TMPFrontiersNoch keine Bewertungen
- tmpD1FE TMPDokument6 SeitentmpD1FE TMPFrontiersNoch keine Bewertungen
- tmpB1BE TMPDokument9 SeitentmpB1BE TMPFrontiersNoch keine Bewertungen
- tmp3656 TMPDokument14 Seitentmp3656 TMPFrontiersNoch keine Bewertungen
- tmpA0D TMPDokument9 SeitentmpA0D TMPFrontiersNoch keine Bewertungen
- Tmp75a7 TMPDokument8 SeitenTmp75a7 TMPFrontiersNoch keine Bewertungen
- tmp27C1 TMPDokument5 Seitentmp27C1 TMPFrontiersNoch keine Bewertungen
- tmp2F3F TMPDokument10 Seitentmp2F3F TMPFrontiersNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Panitia Bahasa Inggeris: SK (Felda) Redong, SegamatDokument98 SeitenPanitia Bahasa Inggeris: SK (Felda) Redong, SegamatAishahNoch keine Bewertungen
- 18 Amazing Health Benefits From Honey and CinnamonDokument4 Seiten18 Amazing Health Benefits From Honey and Cinnamongladiola1100% (1)
- Gapan City College Entrepreneurship DepartmentDokument10 SeitenGapan City College Entrepreneurship DepartmentElisha EstiloNoch keine Bewertungen
- Shave 10 Hours Off Your WorkweekDokument50 SeitenShave 10 Hours Off Your WorkweekDimitri PetrovNoch keine Bewertungen
- Project UPLiFT: Teaching Shrimp Paste ProductionDokument14 SeitenProject UPLiFT: Teaching Shrimp Paste Productiondianne caballeroNoch keine Bewertungen
- Nutrition Care PlanDokument10 SeitenNutrition Care Planapi-486925921Noch keine Bewertungen
- Portmafia GroupDokument27 SeitenPortmafia Groupalvinlarano11Noch keine Bewertungen
- THE PROBLEM AND ITS BACKGROUND BackgrounDokument25 SeitenTHE PROBLEM AND ITS BACKGROUND BackgrounRJ DilenNoch keine Bewertungen
- Action PlanDokument8 SeitenAction Planm4ryz4rkNoch keine Bewertungen
- Quiz 5Dokument2 SeitenQuiz 5Kevin TigasNoch keine Bewertungen
- Research Paper - Body ImageDokument13 SeitenResearch Paper - Body Imageapi-495036140Noch keine Bewertungen
- 118 DR Andy Galpin Optimal Nutrition & Supplementation For Fitness Huberman Lab Guest SeriesDokument69 Seiten118 DR Andy Galpin Optimal Nutrition & Supplementation For Fitness Huberman Lab Guest Serieswaheed khanNoch keine Bewertungen
- Lifespan Psychology IGNOUDokument12 SeitenLifespan Psychology IGNOUashish1981Noch keine Bewertungen
- Factors That Affect LongevityDokument7 SeitenFactors That Affect LongevityPhan Thi Thanh LoanNoch keine Bewertungen
- Overnight Oats (Recipe - Tips) - Cookie and KateDokument4 SeitenOvernight Oats (Recipe - Tips) - Cookie and KateNaKituMiNayashiNoch keine Bewertungen
- Primal Testosterone EbookDokument44 SeitenPrimal Testosterone Ebook7nvzs8wn24Noch keine Bewertungen
- Bualaw Also Know Binatog As Is A Common Street Food Found in The PhillpipinesDokument2 SeitenBualaw Also Know Binatog As Is A Common Street Food Found in The PhillpipinesFerimard Brian BorjaNoch keine Bewertungen
- Natural Ramadan Fat Loss PDFDokument4 SeitenNatural Ramadan Fat Loss PDFAhmed KabeerNoch keine Bewertungen
- Hasselback Chicken Recipe - Low Carb, Keto, THM S - Joy Filled EatsDokument2 SeitenHasselback Chicken Recipe - Low Carb, Keto, THM S - Joy Filled EatsCiupi TikNoch keine Bewertungen
- Vegan DietDokument2 SeitenVegan DietAgusteenNoch keine Bewertungen
- The Problem and Its Setting: Page - 1Dokument19 SeitenThe Problem and Its Setting: Page - 1Gabrielle Moise LaranjaNoch keine Bewertungen
- Weekly Meal Planning and Selection and For Special OccasionDokument6 SeitenWeekly Meal Planning and Selection and For Special OccasionNhet Nhet Mercado100% (2)
- Business PlanningDokument51 SeitenBusiness PlanningJustine MadambaNoch keine Bewertungen
- Triptico de Alimentacion SaludableDokument1 SeiteTriptico de Alimentacion Saludablevan_-fryhard0% (1)
- EAP (5) GrammarDokument2 SeitenEAP (5) GrammarDaniBektiSanjayaNoch keine Bewertungen
- Manage Chronic Kidney Disease and Its ComplicationsDokument35 SeitenManage Chronic Kidney Disease and Its ComplicationsTresnanda Bellawana100% (1)
- Enhancement of Biomass Production From Spirulina SPDokument5 SeitenEnhancement of Biomass Production From Spirulina SPmsiregar_38Noch keine Bewertungen
- Real Food Althetes PlateDokument4 SeitenReal Food Althetes Plateapi-236684744Noch keine Bewertungen
- Health Reporting: Winner - Bamuturaki Musinguzi, Daily MonitorDokument14 SeitenHealth Reporting: Winner - Bamuturaki Musinguzi, Daily MonitorAfrican Centre for Media Excellence100% (1)
- Nutritional Needs of Critically Ill PatientsDokument7 SeitenNutritional Needs of Critically Ill Patientstaner_soysurenNoch keine Bewertungen