Das könnte Ihnen auch gefallen
- BANS-184 Important QuestionsDokument31 SeitenBANS-184 Important QuestionsRahul Singh RajputNoch keine Bewertungen
- Unit 4 Epidemiology of Diseases : Environmental HealthDokument21 SeitenUnit 4 Epidemiology of Diseases : Environmental Healthjeet AmarNoch keine Bewertungen
- Kredics Et Al 2015Dokument18 SeitenKredics Et Al 2015Palanisamy ManikandanNoch keine Bewertungen
- Herepes PDFDokument8 SeitenHerepes PDFsuruthiNoch keine Bewertungen
- 2015 PsoriasisDokument12 Seiten2015 PsoriasispablopabloortizortizNoch keine Bewertungen
- Diagnostics 11 00794 v2Dokument11 SeitenDiagnostics 11 00794 v2Adn crnNoch keine Bewertungen
- Etiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyDokument9 SeitenEtiology of Cellulitis and Clinical Prediction of Streptococcal Disease: A Prospective StudyNurul Dwi LestariNoch keine Bewertungen
- Clinically Relevant Mycoses: A Practical ApproachVon EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNoch keine Bewertungen
- EPIDEMIOLOGY LECTURE NOTESDokument88 SeitenEPIDEMIOLOGY LECTURE NOTESHiany Covre de GodoiNoch keine Bewertungen
- Inflammatory DermatosesDokument16 SeitenInflammatory DermatosesArlen ElisaNoch keine Bewertungen
- Tuberculosis Thesis IntroductionDokument8 SeitenTuberculosis Thesis Introductionifywpqvcf100% (2)
- Epidemiology of Allergic Diseases: Adnan CustovicDokument16 SeitenEpidemiology of Allergic Diseases: Adnan Custovicvikas bhallaNoch keine Bewertungen
- Cshperspectmed HFP A019299Dokument14 SeitenCshperspectmed HFP A019299windaNoch keine Bewertungen
- Epidemiology and Outcome ofDokument20 SeitenEpidemiology and Outcome ofrgumralNoch keine Bewertungen
- Definition and Aim of EpidemiologyDokument25 SeitenDefinition and Aim of EpidemiologyJeevan KumarNoch keine Bewertungen
- Molecular Pa Tho GenesisDokument12 SeitenMolecular Pa Tho GenesiskluniversityNoch keine Bewertungen
- Unit 1 Lec InfectiousDokument11 SeitenUnit 1 Lec Infectious2226205Noch keine Bewertungen
- Outbreak Investigations-A PerspectiveDokument7 SeitenOutbreak Investigations-A Perspectivebwchamp1Noch keine Bewertungen
- VPE 321 CompiledDokument199 SeitenVPE 321 CompiledRajesh KumarNoch keine Bewertungen
- IDSA Guidelines for Diagnosis and Management of Skin and Soft-Tissue InfectionsDokument34 SeitenIDSA Guidelines for Diagnosis and Management of Skin and Soft-Tissue InfectionsROSEN NNoch keine Bewertungen
- Epidemiology Measures and ConceptsDokument4 SeitenEpidemiology Measures and ConceptsKyla BuddahimNoch keine Bewertungen
- IDSA Nec FascDokument34 SeitenIDSA Nec FascShameen KhanNoch keine Bewertungen
- WHO CHRON 1966 20 EngDokument7 SeitenWHO CHRON 1966 20 EngCrónicos Jurisdicción J5Noch keine Bewertungen
- Lecture 1Dokument9 SeitenLecture 1Krishnanjali VuNoch keine Bewertungen
- Epidemiology and Clinical Manifestations of Mucormycosis CMIDokument9 SeitenEpidemiology and Clinical Manifestations of Mucormycosis CMIDINESH VENKATESANNoch keine Bewertungen
- Research ArticleDokument7 SeitenResearch ArticleFikri SatriaNoch keine Bewertungen
- Antibiotics and palliative care: managing infections at life's endDokument6 SeitenAntibiotics and palliative care: managing infections at life's endRahmanu ReztaputraNoch keine Bewertungen
- Epidemiology WholeDokument141 SeitenEpidemiology WholeSonali SehrawatNoch keine Bewertungen
- Viral Exanthems in Children: A Great ImitatorDokument14 SeitenViral Exanthems in Children: A Great ImitatorBmNoch keine Bewertungen
- Psoriasis TipeDokument12 SeitenPsoriasis TipeBayu AjieNoch keine Bewertungen
- 29 Nursing Management of Communicable DiseaseDokument79 Seiten29 Nursing Management of Communicable DiseaseMonika SanaaNoch keine Bewertungen
- Atopic Dermatitis Treatment ReviewDokument5 SeitenAtopic Dermatitis Treatment ReviewDewinta OctaNoch keine Bewertungen
- Sociedad Alemana Parte 1Dokument8 SeitenSociedad Alemana Parte 1A Joel ZjNoch keine Bewertungen
- Practice Guidelines For The Diagnosis and Management of Skin and Soft-Tissue InfectionsDokument34 SeitenPractice Guidelines For The Diagnosis and Management of Skin and Soft-Tissue InfectionsNatalia MoranNoch keine Bewertungen
- Howard2019 PDFDokument3 SeitenHoward2019 PDFNazihan Safitri AlkatiriNoch keine Bewertungen
- Cshperspectmed SKN A015354Dokument30 SeitenCshperspectmed SKN A015354Fajr YanuarNoch keine Bewertungen
- Value of Epi Research in Clinical PracticeDokument6 SeitenValue of Epi Research in Clinical PracticeFouzia ShariqNoch keine Bewertungen
- Jurnal Kulit 2Dokument7 SeitenJurnal Kulit 2Reza MardanyNoch keine Bewertungen
- Itch in Elderly People: A Cross-Sectional Study: Investigative ReportDokument9 SeitenItch in Elderly People: A Cross-Sectional Study: Investigative ReportPatricia JesikaNoch keine Bewertungen
- Blistering Disorders: Diagnosis and Treatment: S. W. Y, B A, N S, & A. R ADokument10 SeitenBlistering Disorders: Diagnosis and Treatment: S. W. Y, B A, N S, & A. R ARashmi KumariNoch keine Bewertungen
- Assessment: Infection May Progress To A Life-Threatening Illness If Antibiotic Treatment Is Not GivenDokument28 SeitenAssessment: Infection May Progress To A Life-Threatening Illness If Antibiotic Treatment Is Not GivenCabdiNoch keine Bewertungen
- Bieber, T.Dokument7 SeitenBieber, T.Anak Agung Ayu Ira Kharisma Buana Undiksha 2019Noch keine Bewertungen
- Safari - May 31, 2023 at 955 AMDokument1 SeiteSafari - May 31, 2023 at 955 AMmartinsoladapo19Noch keine Bewertungen
- EpidemiologyDokument7 SeitenEpidemiologyInoxcent MoonNoch keine Bewertungen
- Ana Phy RespiratoryDokument5 SeitenAna Phy Respiratorydayang ranarioNoch keine Bewertungen
- Clinico-Pathologic Conference OutputDokument3 SeitenClinico-Pathologic Conference OutputNorman Vryne CaduaNoch keine Bewertungen
- Vet Pathology GuideDokument166 SeitenVet Pathology GuidemadheshvetNoch keine Bewertungen
- Diagnostic Techniques For Inflammatory Eye Disease: Past, Present and Future: A ReviewDokument10 SeitenDiagnostic Techniques For Inflammatory Eye Disease: Past, Present and Future: A ReviewAyu Ersya WindiraNoch keine Bewertungen
- Cutaneous Tuberculosis - StatPearls - NCBI BookshelfDokument5 SeitenCutaneous Tuberculosis - StatPearls - NCBI BookshelfLinuel Quetua TrinidadNoch keine Bewertungen
- Associated Clinical Factors For Serious Infections in Patients With Systemic Lupus ErythematosusDokument8 SeitenAssociated Clinical Factors For Serious Infections in Patients With Systemic Lupus ErythematosusadeliaputriNoch keine Bewertungen
- This Module: Covers The Knowledge, Skills and AttitudesDokument13 SeitenThis Module: Covers The Knowledge, Skills and AttitudesmeysNoch keine Bewertungen
- Etiopatogênses Artigo ORIGINALDokument33 SeitenEtiopatogênses Artigo ORIGINALLego is LefeNoch keine Bewertungen
- Acute Urticaria in Children: Course of The Disease, Features of Skin MicrobiomeDokument7 SeitenAcute Urticaria in Children: Course of The Disease, Features of Skin MicrobiomeSultan Rahmat SeptianNoch keine Bewertungen
- Psoriasis A Comprehensive Review On The AetiopathoDokument29 SeitenPsoriasis A Comprehensive Review On The AetiopathoGregorius HocevarNoch keine Bewertungen
- Contagion (Movie Review)Dokument5 SeitenContagion (Movie Review)Stephy SalvadorNoch keine Bewertungen
- Ecampus Notes-Topic 9 COMMUNICABLE DISEASES I PDFDokument18 SeitenEcampus Notes-Topic 9 COMMUNICABLE DISEASES I PDFYutman Wa dagoNoch keine Bewertungen
- Epidemiology Study GuideDokument60 SeitenEpidemiology Study GuideTheophilus BaidooNoch keine Bewertungen
- Impetigo and Scabies e Disease Burden and Modern Treatment StrategiesDokument7 SeitenImpetigo and Scabies e Disease Burden and Modern Treatment StrategiesHandy NugrahaNoch keine Bewertungen
- Disease in Population: Learning ObjectivesDokument15 SeitenDisease in Population: Learning ObjectivesSJ JungNoch keine Bewertungen
- Veterinary Epidemiology and Public Health IntroductionDokument6 SeitenVeterinary Epidemiology and Public Health IntroductionHeroNoch keine Bewertungen
- Crispr Technology EssayDokument4 SeitenCrispr Technology Essayhello annyeongNoch keine Bewertungen
- 1st Bio CH 5 McqsDokument4 Seiten1st Bio CH 5 Mcqsanon_768348720Noch keine Bewertungen
- Parainfluenza Viral DiseaseDokument4 SeitenParainfluenza Viral DiseaseJulian Camilo Oviedo NaranjoNoch keine Bewertungen
- DLP Text TypesDokument26 SeitenDLP Text TypesMaryRoseTrinidadNoch keine Bewertungen
- Viral Oncogenesis DR - Fokam-JosephDokument31 SeitenViral Oncogenesis DR - Fokam-JosephRosemary FuanyiNoch keine Bewertungen
- Overview of COVID-19 Disease: Virology, Epidemiology, Prevention Diagnosis, Treatment, and VaccinesDokument39 SeitenOverview of COVID-19 Disease: Virology, Epidemiology, Prevention Diagnosis, Treatment, and Vaccineska waiiNoch keine Bewertungen
- You Cannot Catch Bugs, Germs, Bacteria or Candida - Fungi - Healing Naturally by BeeDokument5 SeitenYou Cannot Catch Bugs, Germs, Bacteria or Candida - Fungi - Healing Naturally by BeePirate CeoNoch keine Bewertungen
- British Horror: 28 Days Later (Danny Boyle, 2002)Dokument12 SeitenBritish Horror: 28 Days Later (Danny Boyle, 2002)Laura RhowbothamNoch keine Bewertungen
- Romeroooooooooooo PDFDokument20 SeitenRomeroooooooooooo PDFLiiseth Alejandra CanchalaNoch keine Bewertungen
- Erythema Multiforme GuideDokument9 SeitenErythema Multiforme Guidenadia salsabilaNoch keine Bewertungen
- Edexcel IAL BIO Question Paper (June 2020)Dokument36 SeitenEdexcel IAL BIO Question Paper (June 2020)Meenakshie Chaudrie50% (2)
- Advanced Drug Delivery ReviewsDokument29 SeitenAdvanced Drug Delivery Reviewslaura martinezNoch keine Bewertungen
- Tropical DiseasesDokument11 SeitenTropical DiseasesMaría José VillaseñorNoch keine Bewertungen
- Sample Questions For Midterm DrillDokument4 SeitenSample Questions For Midterm DrillJulianna Rheaven JoreNoch keine Bewertungen
- Latihan Soal AcEPT UGM 1Dokument25 SeitenLatihan Soal AcEPT UGM 1Nisa Nisa100% (8)
- Classification of Microorganisms: Prokaryotes vs EukaryotesDokument40 SeitenClassification of Microorganisms: Prokaryotes vs EukaryotesRadwa MohamedNoch keine Bewertungen
- Proceeding of The NAVC North American Veterinary Conference: Jan. 13-27, 2007, Orlando, FloridaDokument4 SeitenProceeding of The NAVC North American Veterinary Conference: Jan. 13-27, 2007, Orlando, FloridaLuis SanchezNoch keine Bewertungen
- Hiv/Aids: Foundation Course-1Dokument35 SeitenHiv/Aids: Foundation Course-1Darshan jNoch keine Bewertungen
- Edible Vaccines: Promises and Challenges: Vrinda M Kurup Jaya ThomasDokument12 SeitenEdible Vaccines: Promises and Challenges: Vrinda M Kurup Jaya ThomasBelaNoch keine Bewertungen
- A History of Secret Human Experimentations This Is Compiled From Two Different Sources - 10Dokument9 SeitenA History of Secret Human Experimentations This Is Compiled From Two Different Sources - 10sagor sagor100% (1)
- Diagnostic Virology ProtocolsDokument370 SeitenDiagnostic Virology ProtocolsDaniela Francisca100% (1)
- Section A Multiple-Choice Questions (15 Marks) Answer All QuestionsDokument11 SeitenSection A Multiple-Choice Questions (15 Marks) Answer All Questionsayunna ayunniNoch keine Bewertungen
- Microbiology 2Dokument149 SeitenMicrobiology 2Brian kNoch keine Bewertungen
- Picornaviridae - FMD and Duck Viral HepatitisDokument16 SeitenPicornaviridae - FMD and Duck Viral HepatitisELIJAH EUMIR CUNANANNoch keine Bewertungen
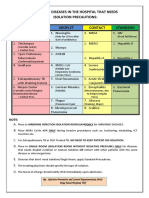
- Common Hospital Diseases Requiring Isolation PrecautionsDokument1 SeiteCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNoch keine Bewertungen
- Generalov-II - Medical Microbiology Virology Immunology - Pt-1 - 2016 PDFDokument282 SeitenGeneralov-II - Medical Microbiology Virology Immunology - Pt-1 - 2016 PDFgmdNoch keine Bewertungen
- FM RegDokument36 SeitenFM RegAnil NaniNoch keine Bewertungen
- Food Safety First LessonDokument101 SeitenFood Safety First LessonJoy Guarte Doron100% (1)
- DBT BET Question Paper 2009 With Answer KeyDokument22 SeitenDBT BET Question Paper 2009 With Answer KeyAbhay Kumar100% (3)
- The Use of Oral Human Grade Ivermectin With Supplements Known As Immunomodulators For Treating Patients With COVID 19 Infections at HomeDokument16 SeitenThe Use of Oral Human Grade Ivermectin With Supplements Known As Immunomodulators For Treating Patients With COVID 19 Infections at HomeAthenaeum Scientific PublishersNoch keine Bewertungen