Das könnte Ihnen auch gefallen
- Presentaton On LBW BabyDokument59 SeitenPresentaton On LBW Babycharanjit kaur100% (1)
- LBWDokument39 SeitenLBWJOSLINNoch keine Bewertungen
- Care of Low Birth Weight BabiesDokument102 SeitenCare of Low Birth Weight Babiesvarshasharma050% (2)
- KANGAROO MOTHER CARE ContentDokument6 SeitenKANGAROO MOTHER CARE ContentAmy Lalringhluani Chhakchhuak100% (2)
- Care of Low Birth WeightDokument21 SeitenCare of Low Birth WeightPrernaSharmaNoch keine Bewertungen
- Priorities List of Nursing DiagnosisDokument4 SeitenPriorities List of Nursing DiagnosisValarmathiNoch keine Bewertungen
- Characteristics of NewbornDokument28 SeitenCharacteristics of NewbornChandu Raj100% (4)
- Case Study On Observation and Newborn CareDokument38 SeitenCase Study On Observation and Newborn CarePiyush Dutta100% (2)
- Care of Child With IncubatorDokument26 SeitenCare of Child With IncubatorSabita Paudel100% (2)
- Nursing Diagnosis Rationale Goals/ Objectives Nursing Intervention S Rational E EvaluationDokument21 SeitenNursing Diagnosis Rationale Goals/ Objectives Nursing Intervention S Rational E EvaluationJoanne Bernadette Aguilar100% (1)
- Care of Low Birth Weight BabiesDokument102 SeitenCare of Low Birth Weight Babiesvarshasharma05100% (1)
- Newborn Appraisal BenitaDokument172 SeitenNewborn Appraisal BenitaBenudavid David100% (2)
- Kangaroo Mother CareDokument6 SeitenKangaroo Mother Careabdullah khalid100% (1)
- Minor Disorders of N.B FinalDokument26 SeitenMinor Disorders of N.B Finalsanthiyasandy67% (3)
- Birth AsphyxiaDokument27 SeitenBirth AsphyxiaJaya Prabha100% (5)
- KMC FinalDokument36 SeitenKMC FinalGandimarei100% (2)
- Phototherapy Care PlanDokument17 SeitenPhototherapy Care PlanSAYMABANU50% (2)
- AyushDokument93 SeitenAyushMamta RajputNoch keine Bewertungen
- Assessment of New BornDokument58 SeitenAssessment of New BornEllen Angel100% (1)
- Nursing Management of Low Birth Weight Baby andDokument30 SeitenNursing Management of Low Birth Weight Baby andArchana100% (2)
- Hydrocephalus N C P BY BHERU LALDokument1 SeiteHydrocephalus N C P BY BHERU LALBheru LalNoch keine Bewertungen
- Pioneer Nursing College Vadodara: Subject: Child Health Nursing Topic: Observation Report (Nicu)Dokument13 SeitenPioneer Nursing College Vadodara: Subject: Child Health Nursing Topic: Observation Report (Nicu)Kinjal Vasava100% (1)
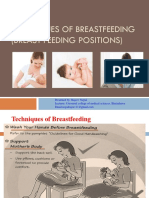
- Technique of Breast Feeding (Position of Breast Feeding)Dokument17 SeitenTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalNoch keine Bewertungen
- Premature LabourDokument29 SeitenPremature LabourSanthosh.S.U100% (1)
- Subinvolution of UterusDokument18 SeitenSubinvolution of Uterusaparna100% (2)
- Antenatal ExercisesDokument8 SeitenAntenatal ExercisesedrinsneNoch keine Bewertungen
- Nursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationDokument4 SeitenNursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationPabhat Kumar50% (2)
- Health Education For Antenatal WomenDokument1 SeiteHealth Education For Antenatal Womenpriyanka100% (1)
- Mechanism of LabourDokument15 SeitenMechanism of Labourangel panchalNoch keine Bewertungen
- ReportDokument20 SeitenReportAshwini Patil0% (1)
- Lesson Plan On Umbilical Cord CareDokument9 SeitenLesson Plan On Umbilical Cord CareJasmine PraveenNoch keine Bewertungen
- Cephalo Pelvic DispoportionDokument12 SeitenCephalo Pelvic DispoportionN. Siva100% (1)
- Asphyxia NeonatorumDokument28 SeitenAsphyxia NeonatorumAsha jilu100% (1)
- Icterus Neonatorum/ Jaundice: 07/12/2021 Rupinder DeolDokument83 SeitenIcterus Neonatorum/ Jaundice: 07/12/2021 Rupinder DeolShivangi SharmaNoch keine Bewertungen
- Nursing Diagnosis Rationale Goals/ Objectives Nursing Interventions Rationale EvaluationDokument20 SeitenNursing Diagnosis Rationale Goals/ Objectives Nursing Interventions Rationale EvaluationElaine Grace Timbol-Babasa100% (1)
- Management of LBW BabiesDokument67 SeitenManagement of LBW BabiesEllen Angel100% (4)
- Birth AsphyxiaDokument2 SeitenBirth AsphyxiaTeslim Raji100% (3)
- Assignment On NicuDokument24 SeitenAssignment On NicuRupali Arora67% (3)
- Health Education On Breast FeedingDokument10 SeitenHealth Education On Breast FeedingSoumya Rajeswari100% (3)
- Artificial Feeding MethodsDokument9 SeitenArtificial Feeding MethodsSAYMABANU100% (1)
- Health Talk On KMCDokument15 SeitenHealth Talk On KMCASHISH KUMAR YADAV100% (8)
- Essential Newborn CareDokument8 SeitenEssential Newborn CareAnnapurna Dangeti100% (1)
- 2 Substitutes For Non-Vegetarian FoodsDokument30 Seiten2 Substitutes For Non-Vegetarian FoodsChinju Cyril100% (1)
- BibliographyDokument6 SeitenBibliographyPiyush DuttaNoch keine Bewertungen
- Newborn Adaptation FinalDokument28 SeitenNewborn Adaptation Finalsanthiyasandy91% (11)
- Balanced DietDokument40 SeitenBalanced DietAkshatha ShivNoch keine Bewertungen
- Postnatal Diet Health TalkDokument13 SeitenPostnatal Diet Health TalkRDi J100% (2)
- Newborn Hypothermia and Hyperthermia (Final Copy)Dokument30 SeitenNewborn Hypothermia and Hyperthermia (Final Copy)Shizuka Marycris Amane67% (3)
- PhototherapyDokument26 SeitenPhototherapyJOSLIN0% (1)
- 13 Assignment-on-PhototherapyDokument11 Seiten13 Assignment-on-Phototherapyamit100% (6)
- Care of Baby Under PhototherapyDokument4 SeitenCare of Baby Under PhototherapyMary Menu100% (1)
- HyperbilirubinemiaDokument10 SeitenHyperbilirubinemiachiboogs456100% (1)
- Female Pelvis and MeasurementsDokument21 SeitenFemale Pelvis and MeasurementsBia KhanNoch keine Bewertungen
- Nicu Physical LayoutDokument16 SeitenNicu Physical LayoutMeena Koushal100% (5)
- Health Teaching During PergnancyDokument4 SeitenHealth Teaching During PergnancyAnuradha MauryaNoch keine Bewertungen
- Lesson Plan On Minor Disorder On NewbornDokument25 SeitenLesson Plan On Minor Disorder On Newbornanjali ahukla92% (12)
- Preterm FinalDokument50 SeitenPreterm Finalsanthiyasandy67% (3)
- The Low Birth Weight Infant: Julniar M Tasli Herman BermawiDokument42 SeitenThe Low Birth Weight Infant: Julniar M Tasli Herman BermawiJoNoch keine Bewertungen
- Topic 2 - Problems Related To Maturity SGA LGADokument60 SeitenTopic 2 - Problems Related To Maturity SGA LGAwydiake3Noch keine Bewertungen
- Care of Iugr and Low Birth Weight BabiesDokument30 SeitenCare of Iugr and Low Birth Weight BabiesjessyNoch keine Bewertungen
- Fkyf 78 of 8 P 888 YyyyyyyyyyyyyyyyyyyyyyyyyyyyyuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuDokument1 SeiteFkyf 78 of 8 P 888 YyyyyyyyyyyyyyyyyyyyyyyyyyyyyuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuAnnisa YusufNoch keine Bewertungen
- Individu TugasDokument1 SeiteIndividu TugasAnnisa YusufNoch keine Bewertungen
- Tugas Individu InggrisDokument8 SeitenTugas Individu InggrisAnnisa YusufNoch keine Bewertungen
- Grammatical Rule 1Dokument47 SeitenGrammatical Rule 1Annisa YusufNoch keine Bewertungen
- Ehgekwfhiurfnrj Ugfreijgnlerljkhbj4n RJGBHTJGNDokument1 SeiteEhgekwfhiurfnrj Ugfreijgnlerljkhbj4n RJGBHTJGNAnnisa YusufNoch keine Bewertungen
- Transient Tachypnea of The Newborn: BackgroundDokument9 SeitenTransient Tachypnea of The Newborn: BackgroundAnnisa YusufNoch keine Bewertungen
- Baby DedicationDokument3 SeitenBaby DedicationLouriel Nopal100% (3)
- An Introduction To Routine and Special StainingDokument13 SeitenAn Introduction To Routine and Special StainingBadiu ElenaNoch keine Bewertungen
- Details Philippine Qualifications FrameworkDokument6 SeitenDetails Philippine Qualifications FrameworkCeline Pascual-RamosNoch keine Bewertungen
- Evan Lagueux - H Argument EssayDokument7 SeitenEvan Lagueux - H Argument Essayapi-692561087Noch keine Bewertungen
- S4 Computer Sciences Exercises PDFDokument2 SeitenS4 Computer Sciences Exercises PDFHenriette Desanges UwayoNoch keine Bewertungen
- Design of Purlins: Try 75mm X 100mm: Case 1Dokument12 SeitenDesign of Purlins: Try 75mm X 100mm: Case 1Pamela Joanne Falo AndradeNoch keine Bewertungen
- The Handmaid's TaleDokument40 SeitenThe Handmaid's Taleleher shahNoch keine Bewertungen
- Module 5Dokument14 SeitenModule 5shin roseNoch keine Bewertungen
- Book Chapter 11 SubmissionDokument18 SeitenBook Chapter 11 Submissioncristine_2006_g5590Noch keine Bewertungen
- PretestDokument8 SeitenPretestAlmonte Aira LynNoch keine Bewertungen
- Eng03 Module Co4Dokument14 SeitenEng03 Module Co4Karl Gabriel ValdezNoch keine Bewertungen
- Swot Analysis of Indian EconomyDokument2 SeitenSwot Analysis of Indian EconomymyeyesrbeautNoch keine Bewertungen
- Project Analysis - M5 - MotorwayDokument6 SeitenProject Analysis - M5 - MotorwayMuhammad Haroon ArshadNoch keine Bewertungen
- Charles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)Dokument441 SeitenCharles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)joan82% (17)
- Effects of Corneal Scars and Their Treatment With Rigid Contact Lenses On Quality of VisionDokument5 SeitenEffects of Corneal Scars and Their Treatment With Rigid Contact Lenses On Quality of VisionJasmine EffendiNoch keine Bewertungen
- Microsome S9 Prep ProtocolDokument22 SeitenMicrosome S9 Prep ProtocolSAN912Noch keine Bewertungen
- Ec 0301Dokument25 SeitenEc 0301Silvio RomanNoch keine Bewertungen
- Furniture AnnexDokument6 SeitenFurniture AnnexAlaa HusseinNoch keine Bewertungen
- Bearing 1Dokument27 SeitenBearing 1desalegn hailemichaelNoch keine Bewertungen
- Machine Design 2021 Guidelines and MechanicsDokument2 SeitenMachine Design 2021 Guidelines and Mechanicsreneil llegueNoch keine Bewertungen
- Masking Conventional Metallic Cast Post For Enhancing EstheticsDokument5 SeitenMasking Conventional Metallic Cast Post For Enhancing EstheticsleilyanisariNoch keine Bewertungen
- FS 1 Episode 2Dokument6 SeitenFS 1 Episode 2Jayson Garcillan UmipigNoch keine Bewertungen
- Sistemas de Mando CST Cat (Ing)Dokument12 SeitenSistemas de Mando CST Cat (Ing)Carlos Alfredo LauraNoch keine Bewertungen
- Defining The Standards For Medical Grade Honey PDFDokument12 SeitenDefining The Standards For Medical Grade Honey PDFLuis Alberto GarcíaNoch keine Bewertungen
- 3-Phase Short-Circuit Current (Isc) at Any Point Within A LV Installation - Electrical Installation GuideDokument6 Seiten3-Phase Short-Circuit Current (Isc) at Any Point Within A LV Installation - Electrical Installation GuideYuukinoriNoch keine Bewertungen
- Rare Watches (Christie's) 16. 05. 2016.Dokument236 SeitenRare Watches (Christie's) 16. 05. 2016.Simon LászlóNoch keine Bewertungen
- Pipe Freezing StudyDokument8 SeitenPipe Freezing StudymirekwaznyNoch keine Bewertungen
- UserProvisioningLabKit 200330 093526Dokument10 SeitenUserProvisioningLabKit 200330 093526Vivian BiryomumaishoNoch keine Bewertungen
- LAB REPORT - MGCLDokument5 SeitenLAB REPORT - MGCLKali stringsNoch keine Bewertungen
- Industrial Motor Control Part IDokument38 SeitenIndustrial Motor Control Part Ikibrom atsbha100% (2)