Das könnte Ihnen auch gefallen
- Contemporary Issues in Child Welfare PracticeVon EverandContemporary Issues in Child Welfare PracticeHelen CahalaneNoch keine Bewertungen
- Systematic Review of Interventions Used in or Relevant To Occupational Therapy For Children With Feeding Difficulties Ages Birth-5 YearsDokument8 SeitenSystematic Review of Interventions Used in or Relevant To Occupational Therapy For Children With Feeding Difficulties Ages Birth-5 YearsGabriela LalaNoch keine Bewertungen
- Sensorimotor Intervention Group For Children With ADHD and Sensory Processing Dif Ficulties: A Feasibility StudyDokument13 SeitenSensorimotor Intervention Group For Children With ADHD and Sensory Processing Dif Ficulties: A Feasibility StudyMageeNoch keine Bewertungen
- A Demonstration of Caregiver Implemented Functional Analysis of Inappropriate Mealtime Behavior Via Telehealth (2021)Dokument6 SeitenA Demonstration of Caregiver Implemented Functional Analysis of Inappropriate Mealtime Behavior Via Telehealth (2021)evellynNoch keine Bewertungen
- E014158 FullDokument11 SeitenE014158 FullSusi RutmalemNoch keine Bewertungen
- A Randomized Controlled Trial of Pivotal Response Treatment Group For Parents of Children With AutismDokument9 SeitenA Randomized Controlled Trial of Pivotal Response Treatment Group For Parents of Children With AutismAlexandra DragomirNoch keine Bewertungen
- Promoting Mealtime Function in People With Dementia: A Systematic Review of Studies Undertaken in Residential Aged CareDokument20 SeitenPromoting Mealtime Function in People With Dementia: A Systematic Review of Studies Undertaken in Residential Aged CaremalnatsNoch keine Bewertungen
- Debbie BromleyDokument5 SeitenDebbie Bromleynurharyanti darmaningtyasNoch keine Bewertungen
- Stern 2016Dokument19 SeitenStern 2016Monalisa CostaNoch keine Bewertungen
- BST 2Dokument12 SeitenBST 2Fernanda ClaudinoNoch keine Bewertungen
- Healthy Habits, Happy Homes Randomized Trial To Improve Household Routines For Obesity Prevention Among Preschool-Aged ChildrenDokument8 SeitenHealthy Habits, Happy Homes Randomized Trial To Improve Household Routines For Obesity Prevention Among Preschool-Aged ChildrenRiftiani NurlailiNoch keine Bewertungen
- Kegunaan Bahan BangunanDokument11 SeitenKegunaan Bahan BangunanyofitaNoch keine Bewertungen
- Incontinencia Fecal PDFDokument6 SeitenIncontinencia Fecal PDFLuisa duenasNoch keine Bewertungen
- Reducing Tube Feeds and TongueDokument9 SeitenReducing Tube Feeds and Tongueszeho chanNoch keine Bewertungen
- Assessment of Pediatric DysphagiaDokument10 SeitenAssessment of Pediatric DysphagiaPamela Tamara Fernández EscobarNoch keine Bewertungen
- 2007 FoodNutrBull 375 RoySKDokument9 Seiten2007 FoodNutrBull 375 RoySKhafsatsaniibrahimmlfNoch keine Bewertungen
- 1 s2.0 S0195666318302605 MainDokument9 Seiten1 s2.0 S0195666318302605 MainmiraandrianiNoch keine Bewertungen
- Ipp Synthesis Table-3Dokument6 SeitenIpp Synthesis Table-3api-707154821Noch keine Bewertungen
- Treating Rural Pediatric Obesity Through Telemedicine: Baseline Data From A Randomized Controlled TrialDokument9 SeitenTreating Rural Pediatric Obesity Through Telemedicine: Baseline Data From A Randomized Controlled Trialapi-546998503Noch keine Bewertungen
- EAT UP Family Centered Feeding InterventDokument15 SeitenEAT UP Family Centered Feeding InterventAndrea Díaz RodríguezNoch keine Bewertungen
- Muliika StephenDokument12 SeitenMuliika StephenLiikascypherNoch keine Bewertungen
- ArticuloDokument9 SeitenArticuloKarol IcNoch keine Bewertungen
- Ebp Early Implementation of Pediatric Palliative Care PetersonDokument1 SeiteEbp Early Implementation of Pediatric Palliative Care Petersonapi-742879730Noch keine Bewertungen
- A Call To Reexamine Quality of Life Through Relationship-Based FeedingDokument7 SeitenA Call To Reexamine Quality of Life Through Relationship-Based FeedingLauraNoch keine Bewertungen
- Measuring Costs and Outcomes of Tele-Intervention When Serving Families of Children Who Are Deaf/Hard-of-HearingDokument8 SeitenMeasuring Costs and Outcomes of Tele-Intervention When Serving Families of Children Who Are Deaf/Hard-of-HearinganaNoch keine Bewertungen
- Maternal Child Nutrition - 2022 - Vilar Compte - Impact of Baby Behaviour On Caregiver S Infant Feeding Decisions DuringDokument11 SeitenMaternal Child Nutrition - 2022 - Vilar Compte - Impact of Baby Behaviour On Caregiver S Infant Feeding Decisions DuringMagaly GalvezNoch keine Bewertungen
- McKee M, 2019Dokument9 SeitenMcKee M, 2019Anibal LeNoch keine Bewertungen
- Sanders 2010Dokument8 SeitenSanders 2010yawnerNoch keine Bewertungen
- 4 Family-Centered Early Intervention For Children With Disabilities Provided Through TelepracticeDokument24 Seiten4 Family-Centered Early Intervention For Children With Disabilities Provided Through TelepracticeJanice Cheuk Yin LoNoch keine Bewertungen
- AlimentaciónDokument23 SeitenAlimentaciónMaro LisNoch keine Bewertungen
- BST + Seletividade AlimentarDokument16 SeitenBST + Seletividade AlimentarVinicius MartinsNoch keine Bewertungen
- Evidence To Support Treatment Options For Children With Swallowing and Feeding Disorders: A Systematic ReviewDokument31 SeitenEvidence To Support Treatment Options For Children With Swallowing and Feeding Disorders: A Systematic ReviewPastoral Duoc Puente AltoNoch keine Bewertungen
- Abigail Kennedy Et Al. - Improving Novel Food Choices in Preschool Children Using Acceptance and Commitment TherapyDokument8 SeitenAbigail Kennedy Et Al. - Improving Novel Food Choices in Preschool Children Using Acceptance and Commitment TherapyIrving Pérez MéndezNoch keine Bewertungen
- Acceptance and Commitment Therapy For Women Diagnosed With Binge EatingDokument12 SeitenAcceptance and Commitment Therapy For Women Diagnosed With Binge EatingPamela MaercovichNoch keine Bewertungen
- Research Day-Nidcap - Goddard & Noss 2015Dokument16 SeitenResearch Day-Nidcap - Goddard & Noss 2015api-262531856Noch keine Bewertungen
- Current Research in Nutrition and Food ScienceDokument8 SeitenCurrent Research in Nutrition and Food Sciencenewbire vlogNoch keine Bewertungen
- Artículo ReferenciaDokument15 SeitenArtículo ReferenciamuskanbasNoch keine Bewertungen
- Assessment of Pediatric Dysphagia and Feeding Disorders: Clinical and Instrumental ApproachesDokument12 SeitenAssessment of Pediatric Dysphagia and Feeding Disorders: Clinical and Instrumental ApproachesAldo Hip NaranjoNoch keine Bewertungen
- SciencedirectDokument14 SeitenSciencedirectHilda RiveraNoch keine Bewertungen
- 00385-HHS-2007-ACF-ACYF-CU-0022 CFDokument1 Seite00385-HHS-2007-ACF-ACYF-CU-0022 CFlosangelesNoch keine Bewertungen
- Effectiveness of A Home Program IntervenDokument8 SeitenEffectiveness of A Home Program IntervenMaria MadalinaNoch keine Bewertungen
- 2018, Parent-Implemented Interventions Around The GlobeDokument25 Seiten2018, Parent-Implemented Interventions Around The GlobeLaisy LimeiraNoch keine Bewertungen
- Determinants of Parent Delivered Therapy Interventions in Children With Cerebral Palsy: A Qualitative Synthesis and ChecklistDokument11 SeitenDeterminants of Parent Delivered Therapy Interventions in Children With Cerebral Palsy: A Qualitative Synthesis and Checklistying reenNoch keine Bewertungen
- Children and Youth Services Review: Mairead Furlong, Fergal Mcloughlin, Sinead McgillowayDokument11 SeitenChildren and Youth Services Review: Mairead Furlong, Fergal Mcloughlin, Sinead McgillowayTere OliverosNoch keine Bewertungen
- Child Development - 2011 - Lowell - A Randomized Controlled Trial of Child FIRST A Comprehensive Home Based InterventionDokument16 SeitenChild Development - 2011 - Lowell - A Randomized Controlled Trial of Child FIRST A Comprehensive Home Based InterventionCláudia Isabel SilvaNoch keine Bewertungen
- FNCP - MalnutritionDokument3 SeitenFNCP - MalnutritionoctoberttwentythreeNoch keine Bewertungen
- BagusDokument12 SeitenBagusmerawatidyahsepitaNoch keine Bewertungen
- UNIDAD 4 Paper Hiperresponsivo y Control EsfinteresDokument8 SeitenUNIDAD 4 Paper Hiperresponsivo y Control EsfinteresCarla Gutierrez Villagrán - Colegio EtchegoyenNoch keine Bewertungen
- Beaudry Lane 2017 SOR RFI Ver PDFDokument8 SeitenBeaudry Lane 2017 SOR RFI Ver PDFcLAUDIANoch keine Bewertungen
- Effectiveness of Community-Based Early Intervention For Childrens With Autism Spectrum Disorder. A Meta-AnalysisDokument10 SeitenEffectiveness of Community-Based Early Intervention For Childrens With Autism Spectrum Disorder. A Meta-AnalysisLucas De Almeida MedeirosNoch keine Bewertungen
- Capacitación para Padres para Niños Con o en Riesgo de Retraso en El Desarrollo El Papel de Completar La Tarea de Los Padres 2016Dokument13 SeitenCapacitación para Padres para Niños Con o en Riesgo de Retraso en El Desarrollo El Papel de Completar La Tarea de Los Padres 2016GLORIA URREANoch keine Bewertungen
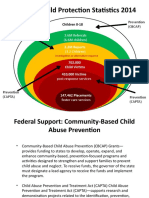
- National Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)Dokument14 SeitenNational Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)MarryRose Dela Torre FerrancoNoch keine Bewertungen
- The Healthy Kids & Families StudyDokument8 SeitenThe Healthy Kids & Families StudyE192Rahmania N. SabitahNoch keine Bewertungen
- Supporting The Transition To Parenthood: Development of A Group Health-Promoting ProgrammeDokument11 SeitenSupporting The Transition To Parenthood: Development of A Group Health-Promoting ProgrammeIonela BogdanNoch keine Bewertungen
- Program Components of Psychosocial Interventions in Foster and Kinship Care: A Systematic ReviewDokument28 SeitenProgram Components of Psychosocial Interventions in Foster and Kinship Care: A Systematic ReviewFLAVIAOLIVARESNoch keine Bewertungen
- 1 s2.0 S0190740915000870 Main PDFDokument7 Seiten1 s2.0 S0190740915000870 Main PDFYusranNoch keine Bewertungen
- Prevention - of - Childhood - Obesity - A - Position - Paper - EAT RIGHT 2022Dokument20 SeitenPrevention - of - Childhood - Obesity - A - Position - Paper - EAT RIGHT 2022MarianaNoch keine Bewertungen
- Family Nursing Care Plan: Nursing Interventions Rationale Methods of Nurse-Family Contact Resources RequiredDokument2 SeitenFamily Nursing Care Plan: Nursing Interventions Rationale Methods of Nurse-Family Contact Resources RequiredAlma Cayap100% (1)
- EBN EmyDokument12 SeitenEBN EmyEileen CeloricoNoch keine Bewertungen
- ABA Analysis AutismDokument15 SeitenABA Analysis Autismasmita sainiNoch keine Bewertungen
- Agency Canvas Ing PresentationDokument27 SeitenAgency Canvas Ing Presentationkhushi jaiswalNoch keine Bewertungen
- To Study Customer Relationship Management in Big BazaarDokument45 SeitenTo Study Customer Relationship Management in Big BazaarAbhi KengaleNoch keine Bewertungen
- HSCC SRH 0705 PDFDokument1 SeiteHSCC SRH 0705 PDFBhawna KapoorNoch keine Bewertungen
- Aliping PDFDokument54 SeitenAliping PDFDirect LukeNoch keine Bewertungen
- Komunikasi Sebagai Piranti Kebijakan Bi: Materi SESMABI Mei 2020Dokument26 SeitenKomunikasi Sebagai Piranti Kebijakan Bi: Materi SESMABI Mei 2020syahriniNoch keine Bewertungen
- Instructions For Preparing Manuscript For Ulunnuha (2019 Template Version) Title (English and Arabic Version)Dokument4 SeitenInstructions For Preparing Manuscript For Ulunnuha (2019 Template Version) Title (English and Arabic Version)Lailatur RahmiNoch keine Bewertungen
- 10 Killer Tips For Transcribing Jazz Solos - Jazz AdviceDokument21 Seiten10 Killer Tips For Transcribing Jazz Solos - Jazz Advicecdmb100% (2)
- SABRE MK-3 CFT Gel SpecDokument1 SeiteSABRE MK-3 CFT Gel Specseregio12Noch keine Bewertungen
- Alternative Network Letter Vol 7 No.1-Apr 1991-EQUATIONSDokument16 SeitenAlternative Network Letter Vol 7 No.1-Apr 1991-EQUATIONSEquitable Tourism Options (EQUATIONS)Noch keine Bewertungen
- Iaea Tecdoc 1092Dokument287 SeitenIaea Tecdoc 1092Andres AracenaNoch keine Bewertungen
- EN 50122-1 January 2011 Corrientes RetornoDokument81 SeitenEN 50122-1 January 2011 Corrientes RetornoConrad Ziebold VanakenNoch keine Bewertungen
- Santu BabaDokument2 SeitenSantu Babaamveryhot0950% (2)
- Editan - Living English (CD Book)Dokument92 SeitenEditan - Living English (CD Book)M Luthfi Al QodryNoch keine Bewertungen
- Colorfastness of Zippers To Light: Standard Test Method ForDokument2 SeitenColorfastness of Zippers To Light: Standard Test Method ForShaker QaidiNoch keine Bewertungen
- T5 B11 Victor Manuel Lopez-Flores FDR - FBI 302s Re VA ID Cards For Hanjour and Almihdhar 195Dokument11 SeitenT5 B11 Victor Manuel Lopez-Flores FDR - FBI 302s Re VA ID Cards For Hanjour and Almihdhar 1959/11 Document Archive100% (2)
- Introduction To Atomistic Simulation Through Density Functional TheoryDokument21 SeitenIntroduction To Atomistic Simulation Through Density Functional TheoryTarang AgrawalNoch keine Bewertungen
- C4 Vectors - Vector Lines PDFDokument33 SeitenC4 Vectors - Vector Lines PDFMohsin NaveedNoch keine Bewertungen
- EdisDokument227 SeitenEdisThong Chan100% (1)
- 385C Waw1-Up PDFDokument4 Seiten385C Waw1-Up PDFJUNA RUSANDI SNoch keine Bewertungen
- 788 ManualDokument16 Seiten788 Manualn0rdNoch keine Bewertungen
- Moquerio - Defense Mechanism ActivityDokument3 SeitenMoquerio - Defense Mechanism ActivityRoxan MoquerioNoch keine Bewertungen
- Comparison of PubMed, Scopus, Web of Science, and Google Scholar - Strengths and WeaknessesDokument5 SeitenComparison of PubMed, Scopus, Web of Science, and Google Scholar - Strengths and WeaknessesMostafa AbdelrahmanNoch keine Bewertungen
- Ajmera - Treon - FF - R4 - 13-11-17 FinalDokument45 SeitenAjmera - Treon - FF - R4 - 13-11-17 FinalNikita KadamNoch keine Bewertungen
- What Is Universe?Dokument19 SeitenWhat Is Universe?Ruben M. VerdidaNoch keine Bewertungen
- Gomez-Acevedo 2010 Neotropical Mutualism Between Acacia and Pseudomyrmex Phylogeny and Divergence TimesDokument16 SeitenGomez-Acevedo 2010 Neotropical Mutualism Between Acacia and Pseudomyrmex Phylogeny and Divergence TimesTheChaoticFlameNoch keine Bewertungen
- Babe Ruth Saves BaseballDokument49 SeitenBabe Ruth Saves BaseballYijun PengNoch keine Bewertungen
- Mechanical Engineering - Workshop Practice - Laboratory ManualDokument77 SeitenMechanical Engineering - Workshop Practice - Laboratory Manualrajeevranjan_br100% (4)
- 1B20 40Dokument4 Seiten1B20 40Electrival TcatallerNoch keine Bewertungen
- Bajaj Vs Hero HondaDokument63 SeitenBajaj Vs Hero HondaHansini Premi100% (1)
- This Study Resource Was: For The Next 6 ItemsDokument9 SeitenThis Study Resource Was: For The Next 6 ItemsJames CastañedaNoch keine Bewertungen