Beruflich Dokumente
Kultur Dokumente
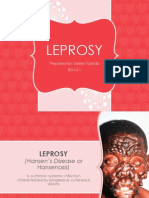
Lepraaa
Hochgeladen von
Ieien MuthmainnahOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Lepraaa
Hochgeladen von
Ieien MuthmainnahCopyright:
Verfügbare Formate
TMIH572
Tropical Medicine and International Health
volume 5 no 6 pp 388399 june 2000
Review: Mycobacterium leprae millennium resistant!
Leprosy control on the threshold of a new era
Jan Visschedijk1, Jacques van de Broek1, Henk Eggens1, Peter Lever1, Stella van Beers2 and Paul Klatser2
1 Department of Health Care and Disease Control, Royal Tropical Institute, Amsterdam, The Netherlands
2 Department of Biomedical Research, Royal Tropical Institute, Amsterdam, The Netherlands
Summary Over the past decades, the conditions of leprosy control implementation have changed dramatically.
Introduction of multidrug therapy, together with the global effort of the World Health Organization to
eliminate leprosy as a public health problem, had a tremendous impact on leprosy control, particularly by
decreasing the registered prevalence of the disease. At the beginning of the new millennium, leprosy control
programmes face several new challenges. These relate not only to changes in the prevalence of the disease,
but also to changes in the context of leprosy control, such as those created by health sector reforms and
other disease control programmes. This review discusses current knowledge on the epidemiology of
Mycobacterium leprae and some important aspects of leprosy control. It is argued that our understanding is
still insufficient and that, so far, no consistent evidence exists that the transmission of leprosy has been
substantially reduced. Sustainable leprosy control, rather than elimination, should be our goal for the
foreseeable future, which also includes care for patients on treatment and for those released from treatment.
This, however, requires new strategies.
keywords leprosy control, leprosy elimination
correspondence Jan Visschedijk, Royal Tropical Institute, Health Care and Disease Control,
Wibautstraat 137J, 1097 DN Amsterdam, The Netherlands. E-mail: j.visschedijk@kit.nl
Introduction Epidemiology
Throughout history, leprosy has been characterized as a disease Transmission
responsible for serious deformities and disabilities resulting in Though Mycobacterium leprae was one of the first
stigmatization and psychological and social suffering. Though microorganisms directly associated with a specific disease,
leprosy has been prevalent in most parts of the world, it large gaps still exist in our knowledge (WHO 1998a). This
vanished in several areas, including northern Europe, long applies not only to the pathology and immunology, but also to
before an efficacious treatment was developed. However, at the crucial epidemiological aspects. Figure 1 presents a simplified
end of the 20th century, leprosy was still endemic in many model of the transmission of M. leprae, indicating that
developing countries, particularly affecting the poorest infection does not necessarily lead to any symptom or lesion
segments of these societies. Every year more than half a specific for the disease leprosy. In fact, it is assumed that M.
million people are diagnosed as leprosy patients, while millions leprae is not very pathogenic and that most infections do not
suffer from the sequelae of the disease. Hence in 1991 the result in symptoms. Early symptoms of leprosy can be self-
World Health Assembly called for a global effort to eliminate limiting and skin lesions can heal spontaneously (Fine 1982).
leprosy as a public health problem by the end of the second Individuals who suffer from the disease, particularly those
millennium. with multibacillary (MB) leprosy, are sources for spread of the
388 2000 Blackwell Science Ltd
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
1991; Frommel et al. 1994; Kawamua et al. 1994). Also, it is
uncertain whether HIV infection is modifying the expression
or course of M. leprae infection (Sampaio et al. 1995). In
Ethiopia no evidence was found to support an association
between HIV infection and a shift towards multibacillary
disease (Frommel et al. 1994), whereas the seroprevalence of
HIV was higher in MB patients than in PB patients in Uganda
and Tanzania (Borgdorff et al. 1993; Kawuma et al. 1994).
These conflicting results may be explained by confounding
factors (Van Beers et al. 1996). Globally, however, there is no
Figure 1 Transmission cycle of Mycobacterium Leprae. Modified indication as yet that the HIV epidemic is leading to a
after Van Beers et al. (1996). significant increase in the number of leprosy patients. The
impact of HIV on leprosy may be minimal because it simply
takes too much time for an infection of M. leprae to develop
symptoms (Van Beers et al. 1996).
infection. The most important port of entry and exit of M.
Distribution and trends
leprae is the respiratory system, particularly the nose; its
dissemination through skin lesions seems to be less important. Table 1 gives an overview of the registered prevalence in 1999
But what happens to those who are infected but do not develop and case detection rate in 1998, as reported by WHO (1999).
the disease? Do some of them become carriers? And if so, are At the beginning of 1999, more than 800 000 leprosy cases
they an important source in the transmission of the M. leprae? were registered for treatment worldwide. In 1998 a similar
There is increasing evidence from nasal polymerase chain number of new cases was detected. The distribution, however,
reaction (PCR) studies of temporary carriage or even is very uneven. About 75% of the registered patients live in
subclinical infection (Van Beers et al. 1996; Cree & Smith South-east Asia, particularly in India. In 1998, 32 countries
1998) and that infected persons may go through a transient had a leprosy prevalence exceeding 1 case per 10 000
period of nasal excretion, indicating that the mycobacterium is population. In absolute terms the global leprosy burden was
highly infective (Hatta et al. 1995). Patients household concentrated in 16 countries (Table 2), with India as the
contacts, neighbours, and social contacts have an increased absolute number one (WHO 1998b). These national figures,
risk of contracting the disease (Van Beers et al. 1999). Whether however, conceal clustering within countries and significant
this is mainly the result of closer contacts to the index case, differences in prevalence between regions, districts and
similar genetic and immunological background, environmental communities.
factors, or a combination of all these, has still to be resolved. Figure 2 indicates that the registered prevalence has
A crucial factor in the process from infection to disease is decreased dramatically over the last decade, but is currently
the immune status of the host. Research and debate have levelling off (WHO 1998b). Over the same period, however, the
focused on whether and how infections with other case detection rate has been more or less constant for most of
microorganisms may modify the immune response to M.
leprae. It has, for example, been suggested that a previous
infection with Mycobacterium tuberculosis may boost the
immune system, thereby diminishing the chances of developing Table 1 Leprosy cases detected and registered (WHO 1999)
leprosy (Lietman et al. 1997). BCG vaccination provides
Cases detected Registered cases
protection against leprosy, although studies have shown the in 1998 in 1999
degree of protection to vary from 20% to 80% (Fine 1995). (rate per 10 000) (rate per 10 000)
BCG immunization may also be responsible for a shift in
immune response from multibacillary to paucibacillary (PB)
Africa 851 530 (0.8) 868 457 (1.1)
leprosy (Chaudhury et al. 1994; Van Beers et al. 1996). Americas 847 218 (0.6) 886 029 (1,1)
The consequences of an infection with the Human South-East Asia 689 069 (4.7) 635 719 (4.3)
Immunodeficiency Virus (HIV) on the risk of developing Eastern Mediterranean 885923 (0.1) 009748 (0.2)
leprosy remain controversial (Van Beers et al. 1996). Some Western-Pacific 810 617 (0.1) 819 487 (0.1)
studies have suggested an association between HIV infection Europe 804 492 (0.0) 04 4765 (0.0)
and leprosy (Borgdorff et al. 1993; Van den Broek et al. 1997), Total 804 449 (1.4) 820 205 (1.4)
while others did not find any association (Pnnighaus et al.
2000 Blackwell Science Ltd 389
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
Table 2 Cases detected (1998) and registered
Cases Rate per Registered Rate per prevalence (as of 1st January 1998) in 16
detected 10 000 prevalence 10 000 leprosy endemic countries (WHO 1998c)
India 524 411 5.3 527 344 5.3
Brazil 543 933 2.6 572 953 4.3
Indonesia 515 337 0.7 529 225 1.4
Madagascar 511 555 7.1 511 005 6.8
Bangladesh 511 320 0.9 513 248 1.0
Myanmar 559086 1.8 513 581 2.7
Nepal 557446 3.2 512 540 5.3
Nigeria 557176 0.6 512 878 1.1
Guinea 556117 8.4 554805 6.6
Philippines 554942 0.7 558749 1.2
Ethiopia 554444 0.7 558104 1.4
Mozambique 554195 2.4 511 072 6.2
Democratic Republic of Congo 553781 0.8 554863 1.0
Sudan 552633 0.9 554065 1.3
Cambodia 552438 2.2 551921 1.7
Niger 552288 2.3 552738 2.7
the time, although there has been a steady increase since 1995. and particularly prevalence of patients registered for treatment
Though some global trends can be identified, there are (registered prevalence), as the main indicator for the
significant differences between countries. While in some epidemiology of leprosy, has several caveats (Box 1).
countries case detection rates are more or less stable (India), in In principle, incidence is a better measure for monitoring of
others these rates decrease (China) or even increase trends in transmission. However, virtually no information on
(Bangladesh) (Smith 1997). incidence rates exists (Fine 1992; Smith 1997). Case detection
Recently, a lively debate has emerged on the significance of rates (CDR 5 all new cases annually registered in health
these trends (in registered prevalence and case detection rate) facilities) are substantially flawed in functioning as proxy
for the epidemiology of leprosy in general and the indicators for incidence rates. Firstly, not all cases detected are
transmission of M. leprae in particular. The use of prevalence, in actual fact recent new cases. Some ostensibly new cases may
25 Figure 2 Leprosy trend in 32
Case Detection rate endemic countries combined.
Prevalence and case detection rate per 10 000
Prevalence rate
20
15
10
0
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997
390 2000 Blackwell Science Ltd
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
Box 1 Prevalence as the indicator for the elimination of leprosy as a Early detection of patients
public health problem some caveats
Patient delay varies with the level of stigma prevailing in a
Prevalence is highly influenced by the duration of the certain area. Although stigma may have been reduced in
disease. Since in earlier years patients often underwent many countries, it is still considerable in some communities
lifelong treatment, the introduction of multidrug therapy
(Myint et al. 1992; Raju & Kopparty 1995; Croft & Croft
(MDT) has had a profound impact on the duration of the
disease, and thus on the registered prevalence.
1998). Public education and the provision of effective
treatment with multidrug therapy (MDT) play an important
Not the real prevalence is measured but only the registered
role in further reducing the stigma linked with the disease
prevalence. Those who have leprosy, but have not reported
to a health facility are not included in these figures. In (Jopling 1991). (Multidrug therapy (MDT) was introduced
addition, when MDT was introduced in leprosy for leprosy control as a response to increasing resistance to
programmes, patients who had been labelled and registered monotherapy with dapsone. The regimen for PB patients
for a long time as leprosy patients were discharged,
consists of dapsone and rifampicin for six months, while the
including several misdiagnosed cases (Fine 1992).
Furthermore, defaulters are continuously being removed regimen for MB patients consists of dapsone, rifampicin and
from leprosy registers and, thus, not included in registered clofazamin for 12 or 24 months. Patients collect a monthly
prevalence rates. blister pack which contains their daily medication.)
The prevalence measured is the point-prevalence (taken at a Due to the lack of a single independent gold standard for
certain moment in time, e.g. 1st January) and not the diagnosis, the diagnosis of leprosy is based mainly on clinical
period-prevalence. Patients that are treated for leprosy but symptoms. Laboratory techniques (AFB microscopy) were
who have a shorter treatment schedule than one year, may
introduced for a relatively short period of time, but are now
not be included, e.g. PB-patients;
being abandoned in several areas where leprosy is still
Different diagnostic criteria have been used over the years
endemic. However, there is a need for an easy-to-use
for leprosy. Hence inconsistency in case definition and
diagnosis makes comparisons between different control diagnostic test, particularly because leprosy is a relatively rare
programmes and years cumbersome. disease in many countries, with specific knowledge mainly
concentrated at central level and much less at the periphery.
Recently developed immunological and molecular assays
cannot be used as diagnostic tests in routine control
already have suffered from leprosy for several years, but for programmes, because they do not discriminate clearly
various reasons (stigma, inaccessibility of health services, between infection, contamination, and disease (Van Beers
opportunity costs) not visited a health facility. They constitute 1998). However, these tests may be useful for the diagnosis of
the so-called hidden backlog of leprosy cases. Defaulting and subclinical infections and the detection of sources of
re-registering (shopping), as well as relapses may also inflate transmission.
the figures for new cases detected. Secondly, detection of new
cases depends on the method and intensity of case finding.
Adequate treatment
Active case finding is likely to increase the number of newly
detected cases, while a poorly performing programme may Treatment with MDT of all leprosy patients became the
identify only a small proportion of all new cases. Active case official strategy of the WHO in 1982, when widespread
finding may also overestimate incidence rates, since some new resistance to dapsone had to be confronted. Consequently,
cases are self-healing and should be included neither in research focused particularly on the relapse rate of these new
prevalence nor in incidence rates. Consequently, the currently MDT regimens (Cree & Smith 1998). Different definitions
available information is inadequate to anticipate trends in and indicators have been used to describe relapse (rates),
leprosy epidemiology and transmission. Worldwide which has often hampered comparison between studies.
information on the most crucial indicator, incidence, is lacking WHO has defined relapse as a patient who successfully
(Smith 1997), while trends in CDR may be distorted as a result completes an adequate course of MDT, but subsequently
of confounding and bias (Meima et al. 1997). develops new signs and symptoms of the disease during the
surveillance period or thereafter. In general, the number of
leprosy relapses reported in control programmes has been
Leprosy control
low (Becx-Bleumink 1992; Jesudasan et al. 1996a;
Leprosy control has three main strategic components Dasananjali et al. 1997; Li et al. 1997) and well below the
(Feenstra 1994): Early detection of patients, their adequate relapse rates reported in, for instance, tuberculosis control
treatment, and providing comprehensive care for the programmes.
prevention of disabilities and rehabilitation. The 7th WHO Expert Committee on Leprosy considered,
2000 Blackwell Science Ltd 391
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
based on the results of a multicentre double blind trial from impairment) to perform an activity in the matter of
(Grosset 1997; WHO 1997a) with 24 years of follow-up, that within the range considered normal for a human being.
the 24-month MDT regimen for MB-leprosy can be shortened Handicap: A disadvantage resulting from impairment or
to 12 months. The Medico-Social Commission of the disability, that limits or prevents the fulfilment of a role
International Federation of Anti-Leprosy Associations (ILEP) that is normal, depending on age, sex, social and
supported the advice of the WHO Expert Committee, because cultural factors for the individual.
a shortened course would reduce costs for both programme
However, the chain disease-impairment-disability-
and patient, and would reduce the proportion of defaulters
handicap is not a chronological process. Impairment
(ILEP 1998). Fear has been expressed that the relapse rate for
resulting from leprosy always entails at the same time
those with a relatively high bacterial load may be unacceptably
physical, psychological and social consequences and thus
high (Van Brakel et al. 1989; Waters 1998; Lynch 1999).
involves a disability and a handicap. It ranges from the
Nevertheless, most leprosy-endemic countries have
inability to play a normal role at home and in the community
implemented a shortened 12-month MB-MDT regimen within
and meeting normal social obligations to complete alienation
a year after the Committee met.
from society and destitution. Unfortunately, with few
A relatively new development is the introduction of a single
exceptions, the link between impairment, disability and
dose of rifampicin 600 mg plus ofloxacin 400 mg and
handicap has rarely been studied in detail (Van Brakel 1997).
minocycline 100 mg (ROM) as an acceptable and cost-effective
In many concepts describing the burden of disease, including
alternative regimen for the treatment of single-lesion PB
the DALY (Murray & Lopez 1994), the socio-economic
leprosy. A multicentre double blind trial concluded that ROM
impact of leprosy in terms of handicap is, also for reasons of
is almost as effective as standard 6-month WHO PB-MDT in
international comparison, not included.
the treatment of single lesion leprosy (Single Lesion Multi-
Since the consequences of leprosy are physical,
Centre Trial Group 1997). However, questions were raised on
psychological and socio-economical, rehabilitation covering
the methodology of the study (Lockwood 1997). Furthermore,
these aspects should ideally be interrelated and integrated.
the debate should be seen in light of the fact that 80% of all
Physical rehabilitation is a prerequisite for successful socio-
single-lesion PB cases are self-healing (Ekambaram &
economic functioning. Successful coping with impairments
Sithambaram 1977).
and disabilities is an important determinant of motivation for
These days, most control programmes report treatment
preventing their worsening. In practice, however, physical and
completion rates of 6090% for PB patients and 4080% for
socio-economic rehabilitation interventions have often been
MB patients (ILEP 1999). Reasons for nonadherence are
separated.
reported to be economic (costs of transport, opportunity costs
Leprosy control programmes tend to consider only
of monthly clinic visits), as well as social and psychological
physical rehabilitation. In some countries socio-economic
(self-stigma, no improvement of disabilities, mobility).
rehabilitation is covered by the government through social
Unfortunately, results from studies are often inconsistent and
welfare, NGOs or community-based rehabilitation (CBR)
the exact relationship between these factors and compliance
programmes, which address severely deformed and destitute
remains largely obscure (Vadher & Lalljee 1992).
patients living at home or in leprosaria, and may include
vocational training, income-generating projects and charity.
Prevention of disabilities and rehabilitation Most CBR programmes are tailored to specific local needs
and consequently differ from country to country and even
Leprosy patients suffering from disabilities, which may among different areas of the same country (Deepak 1995).
develop before, during or after MDT, are often easily Integrating all aspects of rehabilitation into CBR
recognizable by the characteristic deformities of their eyes, programmes remains a major challenge. However, a CBR
hands and feet. Impairments and disabilities develop in programme cannot substitute all rehabilitation services,
stages, often starting with nerve damage due to neuritis and particularly not those relating to identification of at-risk
leprosy reactions and resulting in the loss of protective patients and prevention of disabilities (Deepak 1995), which
sensation, as well as the loss of muscle strength and require close collaboration between community rehabilitation
autonomic functions. The International Classification of workers and medical staff.
Impairments, Disabilities and Handicaps gives the following
definitions (WHO 1980):
Towards elimination of leprosy by the year 2000
Impairment: any loss or abnormality of psychological,
physiological, or anatomical structure or function. In 1991 the World Health Assembly adopted a resolution to
Disability: any restriction or lack of ability (resulting eliminate leprosy as a public health problem by the year 2000
392 2000 Blackwell Science Ltd
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
(WHO 1991). Elimination was defined as a level of prevalence that MDT, by making highly infectious patients rapidly
below one case per 10 000. Along with this resolution, WHO noninfectious, will have an impact on the transmission of M.
advocated an approach consisting of four elements: Making leprae. This assumption, however, has been challenged (Fine
MDT available at community level, Leprosy Elimination 1992). The degree of its impact, particularly on the incidence
Campaigns (LECs), Special Action Projects, and close of leprosy, is still largely unknown and subject of intensive
monitoring of the impact, particularly through assessing the discussion (WHO 1998d). Reduced prevalence has mainly
prevalence of leprosy. resulted from shorter treatment schedules and clearing of
The approach has been successful in achieving almost registers, not by a decrease in incidence. Nevertheless, WHO
100% MDT coverage. In many countries LECs have resulted is using registered prevalence as the main indicator to
in the detection of a considerable number of cases. Important monitor progress because of the operational difficulties in
elements of the campaigns are training of health workers in measuring incidence.
case finding, educating communities to increase awareness, The postponement of the elimination date to 2005, and the
active case finding and treating patients. In Nepal more than suggestion by WHO that the next five years are necessary to
11 000 new cases were identified during last years national cure the remaining patients and that only a limited number
campaign (Ministry of Health and Nepal Department of of leprosy patients may occur after the year 2005 (as stated
Health Services 1998), while the number of new cases in the in the ILEP/WHO draft Strategic Plan 20002005 and the
previous year was around 7500 (Ministry of Health Nepal Memorandum of Understanding between WHO and
1998). In 1997 and 1998 LECs were held in 29 Indian States Novartis Pharma AG), strengthen the idea that the leprosy
and Union Territories. More than 500 000 health workers problem is on the point of disappearance (Li et al. 1997).
were involved and 454 290 new cases were detected Such an approach is likely to be counterproductive, because it
(Directorate General of Health Services 1999). may have negative consequences for future support, the
Though LECs have indeed yielded a substantial number of funding of research and the implementation of leprosy
new cases and may have reduced the backlog of leprosy cases, control activities (Anonymous 1997). Presently, there is no
some questions have been raised about their cost- basis for confidence that the incidence and the number of
effectiveness, long-term impact and particularly their new leprosy patients detected annually will have been
diagnostic accuracy. The high number of patients detected substantially reduced in all currently endemic areas after the
during these campaigns may indeed indicate a backlog of year 2005, let alone be zero. Hence, leprosy control activities
patients and an underestimation of the leprosy problem, but should not be exclusively directed towards a magic target but
also considerable overdiagnosis and thus diagnostic towards sustainable leprosy control, far into the new
inaccuracy (WHO 1998c). Another concern is case-holding of millennium. This requires new strategies, rather than
patients found through active case finding. Compared to questionable assumptions.
patients who report to health services voluntarily, these
patients may be less motivated to complete treatment, and
New directions for leprosy control
some of them may have limited access to health facilities.
Special Action Projects for the Elimination of Leprosy The introduction of new and relatively short MDT treatment
(SAPEL) are meant to bring MDT to remote areas where schedules, the expected reduction in priority given to leprosy
routine activities are nonexistant or have proven impractical control, as well as ongoing health sector reforms, make it
(no health infrastructure, geographically difficult to access, imperative for national decision-makers to review the policies
refugees, etc.). SAPELs have generally been less successful: and strategies for leprosy control. While leprosy-specific field
they resulted in only a limited number of new cases (WHO staff was often overburdened 20 years ago, when many
1996; Ebenso 1999), have been relatively expensive and had patients were on lifelong treatment, they now have to deal
questionable adherence levels. with substantially lower patient loads.
While millions of patients have been released from MDT However, if the impression is given that the leprosy
and the global registered prevalence has decreased problem has been eliminated, political interest will wane,
substantially, it is likely that in several leprosy-endemic certainly while other diseases such as AIDS, malaria,
countries the elimination target will not be reached. tuberculosis and noncommunicable diseases require
Prevalence rates vary widely within countries and, as a result increasing attention. (The use of the term elimination as a
various regions continue to have relatively high rates. public health problem is often confused with the definition
Nevertheless, the enhanced commitment for the of elimination as was for instance defined during the
elimination target by the year 2000, to be reached by the main Conference on Global Disease Elimination and Eradication
tool for elimination, MDT, has given a strong impetus to as Public Health Strategies, in Atlanta, USA 1998 (Dowdle &
leprosy control (Feenstra 1992). The underlying assumption is Hopkins 1998). Elimination was here defined as a reduction
2000 Blackwell Science Ltd 393
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
to zero of the incidence of a specified disease in a defined Box 2 Major components of a strategy for sustainable leprosy
geographical area as a result of deliberate efforts (Dowdle control
1998). Control was defined as the reduction of disease
incidence, morbidity or mortality to a locally acceptable level Continuation of early case-finding, treatment with MDT
and prevention of disabilities
as result of deliberate efforts; continued measures are
required to maintain the reduction.) Though understandable,
Enhancing cost-effectiveness, sustainability and equity of
leprosy services through integration and combination with
reduced priority for leprosy should not lead to giving no other disease control programmes
priority at all. Many examples in the past, e.g. in the case of Development of tailor-made leprosy control strategies,
tuberculosis and malaria, demonstrate that abandoning related to patient load
disease control programmes altogether has serious Strengthening human resource development and
management
repercussions when such diseases re-emerge.
The context in which disease control programmes are
Strengthening national level
operating is also changing (Green & Jochem 1998). Most
Strengthening services for patients in need of medical and
social rehabilitation
ministries of health are engaged in reforms, whether slow and Stimulating relevant research
incremental or fast and radical. If a disease control
programme takes a passive and defensive attitude towards
these changes and their possible adverse effects, it might well
Enhancing cost-effectiveness, sustainability and equity of
end up losing an opportunity to influence new health sector
leprosy services through integration and combination with
policies.
other disease control programmes
To maintain political commitment is crucial. In this
context, promotion of (ex)patient organizations, capable of As a result of decreasing prevalence (and therefore workload)
pressurizing governments to fulfil their responsibilities, could combined with high costs and health sector reforms, many
be an important activity. In Brazil, for instance, organizations vertical programmes that still exist (e.g. India) will be
of patients, ex-patients and committed individuals have discontinued in the coming years. Instead, in order to be more
gained strength in the past few years. These organizations efficient and cost-effective and enhance accessibility, leprosy
assist regular health services in health education, case finding programmes of the 21st century have to be merged with other
and case holding activities and confront failing leprosy programmes and, preferably, integrated into the general health
services with their poor performance. services. Two components can be distinguished that are
It is essential that the process to change involves all mutually reinforcing:
concerned parties from the start (governments, health Integration at the level where services are provided: This
workers, patients, non governmental organizations, donors, implies that patients should be diagnosed and treated every day
etc.). Workshops involving all stakeholders should develop of the week, close to their homes, by most, if not all, health
guidelines that can serve as a tool for managers and decision- workers. Multipurpose clinics and staff should attend to the
makers who want to review the organization of leprosy curative and preventive needs of leprosy patients. This will
services and to devise a strategy that will make them more enhance the accessibility of leprosy services for all patients and
sustainable (De Coster et al. 1997). A well-defined strategy broaden their possibilities to complete treatment. It will ensure
aimed at efficient, effective and sustainable leprosy control, that leprosy services continue in the decades to come (Feenstra
presented at the right time, is crucial to keeping leprosy on 1993).
the agenda. Major components of this strategy are Integration needs to be supported by a well-organized health
summarized in Box 2. system, particularly through technical support from higher
levels with training, supervision, drugs supply, monitoring and
policy development. The local context will determine the most
Continuation of early case-finding, treatment with MDT and
feasible modality to ensure that leprosy services remain of
prevention of disabilities
good quality. Particularly the combination of leprosy activities
A high coverage of BCG-vaccination, early detection of with tuberculosis has shown to be a promising option. Both
leprosy patients, followed by treatment with MDT and the disease control programmes target chronic diseases and are
prevention of disabilities, will continue to be the cornerstone often traditionally linked; they are based on a public health
of leprosy control in the 21st century. Passive case finding will perspective with similar principles, i.e. aimed at decreasing
remain the most suitable method for early case finding. transmission by early case finding, adequate case-holding and
However, in specific highly endemic areas, where awareness, monitoring. In countries where a model for leprosy control is
patient motivation, and diagnostic procedures are regarded as well-developed, it can be used to enhance or expand
inadequate, active case finding may be pursued. tuberculosis control. In some regions of Nepal, where the
394 2000 Blackwell Science Ltd
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
leprosy control programme is supporting tuberculosis control, approach is rather expensive. Under such circumstances a
the sustainability of leprosy control is enhanced because it cluster approach would be more appropriate. Services,
makes leprosy activities more cost-effective. Such an approach including the training of health workers, are mainly provided
offers good opportunities for countries such as Nigeria, where in the area where the leprosy problem still exists. In Kenya,
leprosy control is relatively well-established but tuberculosis for example, most new patients come from a limited number
control still relatively weak. Currently, combination with of districts, which has consequences for the organization of
tuberculosis control takes place in Tanzania, Nigeria, leprosy services.
Mozambique, Kenya, Ethiopia, and more recently in In low-endemicity situations an outbreak approach is
Indonesia. In other countries leprosy services are combined needed, whereby contacts of the index case are examined.
with dermatological services, e.g. in Vietnam, Laos, China, Procedures should include the verification of diagnosis and
Brazil and Surinam. In some settings it may be possible to hand treatment of the index case and the examination of intensive
over all supportive activities to the general health services, contacts. The community should be informed, and the health
provided, of course, that sufficient attention is given to the staff in the area should be trained in diagnostic skills and
needs of the leprosy control programme and that the general case management. Routinely, the skills of health workers will
health services are of acceptable quality. mainly be limited to suspecting leprosy.
In several countries, integration at the level of service
delivery and the combination of technical support to leprosy
Strengthening human resource development and
and tuberculosis control go hand in hand. In Ethiopia leprosy
management
services are currently integrated in the general health services
at the most peripheral level, while at the same time support to A critical review of essentially required skills at all levels is
this level is strengthened through the combination with important for working towards sustainable services. Since
tuberculosis control. The number of clinics with facilities to multipurpose workers are desirable, required leprosy-related
diagnose and treat leprosy has increased considerably and the skills need to be carefully defined and standardized, while
combined training and supervision for leprosy and tuberculosis excluding nonessential skills. Taking the recent WHO
control increase the cost-effectiveness, and therefore the initiative on the Integrated Management of Childhood Illness
sustainability, of these services. (Lambrecht et al. 1999; Tulloch 1999) as an example, it may
be useful to consider an equivalent approach for
dermatological problems: the integrated management of skin
Developing tailormade leprosy control strategies
diseases. Simple and valid algorithms on the diagnosis and
Cost-effectiveness and sustainability can also be enhanced by management of skin lesions could help the peripheral health
establishing tailormade leprosy control strategies. An
approach needs to be developed that links leprosy control
activities to the epidemiological situation in a country, e.g.
through the use of simple Geographical Information Systems
(GIS). Based on case detection rates, regions could be
categorized as follows:
Regions with high case detection rates (. 10 per 100 000
per year);
Regions with moderate case detection rates (110 per
100 000 per year);
Regions with low case detection rates (, 1 per 100 000
per year).
Traditionally leprosy control has followed a blanket
approach, whereby support was provided to all areas and to
all health service levels, irrespective of the number of
patients. This is still justified where the number of patients is
high and/or more or less evenly geographically distributed.
Ideally, all components of leprosy control should under these
circumstances be integrated into the basic health services, and
staff has to be trained in these components. Figure 3 Ranking of required skills in order of possibilities to
In situations with moderate case detection rates a blanket delegate to peripheral health services.
2000 Blackwell Science Ltd 395
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
worker to come to meaningful decisions and actions, in the form of septic or reconstructive surgery. They should
including those for leprosy. have access to general surgical facilities. Due to stigma, this is
A tailormade leprosy control strategy, depending on the still not the case in several countries.
patient load, will have substantial consequences for the Grouping rehabilitative interventions into packages for
specific level of expertise required. For most endemic settings, specific conditions or groups of disabled persons will
the ability to suspect leprosy and refer (S & R) to a health facilitate the decision-making and referral process, allowing
unit capable of diagnosing and providing treatment is the individual programmes to adjust the contents of the packages
most important skill required for peripheral multipurpose according to their specific requirements. It allows for
health workers. The supervised provision of treatment is transparency in terms of who is responsible for the delivery of
another task that can be delegated to the lowest level. In areas care. Budgets and costs could be related to the number of
with low patient loads, management of nerve damage will registered disabled patients more easily. We propose the
have to be concentrated in health facilities with a larger following packages of interventions
catchment population, e.g. a district hospital serving
200 000500 000. The centres for the treatment of Neuritis package: early diagnosis and treatment of
reactions and neuritis;
complications of leprosy and rehabilitative surgical services
will be even more concentrated. As the number of contacts Self-care package consisting of health education,
provision of protective materials such as footwear,
between health workers and leprosy patients diminishes,
bandages, sunglasses, etc.;
fewer staff will obtain skills in case management and leprosy
control. Figure 3 illustrates a hierarchical list of the required Surgical care package comprising hospitalized ulcer care,
septic surgery, reconstructive surgery and orthopaedic
skills.
footwear;
To maintain minimum awareness of leprosy, leprosy must
be kept in the curricula of (para) medical workers, even under End stage or amputee package including health
education and the provision of prostheses and crutches.
low endemic circumstances. Each leprosy-endemic country
should have at least one centre of excellence for complicated The level at which these packages would be provided
dermatological and surgical patient management. This need depends on factors such as the case detection rate. Socio-
not be a special leprosy hospital, but may well be an economic rehabilitation (SER) of leprosy patients will remain
adequately equipped general hospital. an important issue. Severely deformed and destitute patients
may continue to live in special places such as leprosaria,
though admission to these places should, in general, be
Strengthening services at the national level
discouraged. Community-based rehabilitation, where these
Regardless of the level of endemicity in a country, a well- patients receive the same kind of services as other people
functioning central unit, usually in the Ministry of Health with severe disabilities, is preferable.
(MoH), is necessary. The central unit should be responsible
for policy formulation and technical guidance, technical
training, and planning, monitoring, evaluation. MoH will Stimulating relevant research
need to sustain an international technical exchange of ideas
The fact that registered prevalence is low does not mean that
and experiences. These contacts are of great importance to
research is no longer needed (ILEP 1996). Health system
maintain a sense of cohesion and to facilitate innovation.
research in particular, formulated within the context of
Most endemic countries will want to maintain links with the
specific leprosy control programmes and orientated towards
national and international donor community.
direct action, should be supported. In addition, three areas
MoH should be capable of formulating a long-term health
for further research should be prioritized:
policy embedding disease control policies including leprosy.
This requires, however, that the national disease control units Studies to determine factors influencing the transmission
are equipped with strong skills in policy development, and to understand the impact of interventions on the
communication and negotiation. epidemiology of leprosy. This will also make
mathematical models to assess future trends in the
epidemiology of leprosy more relevant and reliable.
Strengthening services for patients in need of medical and
social rehabilitation
Research to elucidate the factors that cause delay in early
detection and influence health-seeking behaviour. Since
Worldwide, the number of ex-patients with deformities and stigma, health infrastructure, etc., are often context-
disabilities has already surpassed the number of patients in specific, this is an area where health systems research can
need of MDT. Many of these people will need medical care enhance knowledge and develop relevant interventions.
396 2000 Blackwell Science Ltd
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
Research into early diagnosis and shortened treatment on antileprosy vaccines among high-risk household contacts in
schedules should be encouraged, in order to reduce Calcutta metropolis. International Journal of Leprosy 62,
defaulter rates and (opportunity) costs. 389394.
Cree IA & Cairns Smith W (1998) Leprosy transmission and
Research on leprosy reactions and recent nerve damage
mucosal immunity: towards eradication? Leprosy Review 69,
focusing on the development of tools for diagnosis and
112121.
the treatment of such reactions under field conditions,
Croft RP & Croft RA (1998) Knowledge, attitude and practice
e.g. standardization of the use of corticosteriods. regarding leprosy and tuberculosis in Bangladesh. Leprosy Review
70, 3442.
Dasananjali K, Schreuder PAM & Pirayavaraporn C (1997) A study
Conclusion on the effectiveness and safety of the WHO/MDT regimen in
There are still substantial gaps in our knowledge of leprosy Northeast Thailand; a prospective study. 198496. International
transmission and epidemiology. Only when, through further Journal of Leprosy 65, 2836.
De Coster E & Eggens KH et al. (1997) Sustaining leprosy related
research, these gaps are closed, long-term strategies for real
activities. Guidelines for Responding to Change. ILEP.
elimination can be established. Currently, however, the
Deepak S (1995) Editorial Leprosy and Community-Based
changing circumstances, such as a decreasing registered Rehabilitation. Leprosy Review 66, 273276.
prevalence, health sector reforms, a diminished commitment Directorate General of Health Services New Delhi India (1999)
and scarcity of resources, require a fresh look at policies and Report on the Modified Leprosy Elimination Campaign.
strategies for leprosy control. Such a revision requires an Government of India, New Delhi.
active position by decision-makers, because attempting to Dowdle WR & Hopkins D, eds. (1998) The eradication of infectious
carry on as usual is doomed to lead to the evaporation of diseases: report of the Dahlem Workshop on the Eradication of
leprosy control. Infectious Diseases. Wiley, Chichester 1998.
We have provided directions for leprosy control in the Dowle WR (1998) The principles of disease elimination and
eradication. WHO Bulletin 76(S2), 2225.
coming years, which partly build on experiences of the past
Ebenso BE (1999) Results of a 1-year Special Action Project for the
and partly require the development of new approaches.
Elimination of Leprosy (SAPEL) in poorly accessible areas of
Obviously, on the threshold of the new millennium, an Akwa Ibom State, Nigeria. Leprosy Review 70, 5662.
important chapter in the history of leprosy control will be Ekambaram V & Sithambaram M (1977) Self healing in non-
closed. However, it would be far too early to close the whole lepromatous leprosy in the area of the ELEP leprosy Control
book. Project Dharmapuri (Tamil Nadu). Leprosy in India 49, 387392.
Feenstra P (1992) Needs and prospects for epidemiological tools in
leprosy control. Leprosy Review 63, S3S10.
Acknowledgements Feenstra P (1993) Leprosy control through general health services
The authors thank Lex Muller for his intellectual and and/or combined programmes. Leprosy Review 64, 8996.
technical support, Piet Feenstra for his useful comments and Feenstra P (1994) Sustainability of leprosy control services in low
Leonie McCann for her assistance in editing an earlier draft. endemic situations. International Journal of Leprosy 62, 599608.
Fine PEM (1982) Leprosy: the epidemiology of a slow bacterium.
Epidemiological Review 4, 161168.
References Fine PEM (1992) Editorial Reflections on the Elimination of
Leprosy. International Journal of Leprosy 60, 7180.
Anonymous (1997) Leprosy beyond the year 2000 (Editorial). Lancet Fine PEM (1995) Variation in the protection by BCG: Implications
350, 1717. of and for heterologous immunity. Lancet 346, 13391345.
Becx-Bleumink M (1992) Relapses among leprosy patients treated Frommel D, Tekle Haimanot R, Verdier M, Negesse Y, Bulto T &
with multidrug therapy: experiences in the leprosy control Denis F (1994) HIV infection and leprosy; a four-year survey in
programme of the All Africa Leprosy and Rehabilitation Center Ethiopia. Lancet 344, 165166.
(ALERT) in Ethiopia: Practical difficulties with diagnosing Green & Jochem (1998) Sustaining leprosy services in the changing
relapses; operational procedures and criteria for diagnosing context of health sector reform. Leprosy Review 69, 134144.
relapses. International Journal of Leprosy 60, 421435. Grosset J (1997) Whither short course chemotherapy for leprosy?
Bekri W, Gebre S, Mengiste A et al. (1998) Delay in presentation and Indian Journal of Leprosy 69, 119120.
start of treatment in leprosy patients: a case-control study of Hatta M, Van Beers SM, Madjid B, Djumadi A, de Wit MYL &
disabled and non-disabled patients in three different settings in Klatser PR (1995) Spatial distribution and persistence of
Ethiopia. International Journal of Leprosy 66, 19. Mycobacterium leprae nasal carriage among a population in
Borgdorff MW, van den Broek J, Chum HJ et al. (1993) HIV-1 which leprosy is endemic in Indonesia. Transactions of the Royal
infection as a risk factor for leprosy. A case-control study in Society of Tropical Medicine and Hygiene 89, 381385.
Tanzania. International Journal of Leprosy 61, 556562. ILEP (1996) Medical Commission. Priorities for Leprosy Research
Chaudhury S, Hzara SK, Saha B et al. (1994) An eight-year field trial Priorities. ILEP Medical Bulletin No 10, October 1996.
2000 Blackwell Science Ltd 397
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
ILEP (1998) Advice form the ILEP Medico-social Commission. Journal of Leprosy 65, 259272.
Operational Guidelines for the Introduction of New MDT Sampaio EP, Caneshi JRT, Nery JAC et al. (1995) Cellular immune
Regimens for the Treatment of Leprosy. Medical Bulletin, No 14, response to Mycobacterium leprae infection in human
June 1998. immunodeficiency virus-infected individuals. Infection and
ILEP (1999) Annual Report 199899. Financial Support and Analysis Immunity 63, 18481854.
of ILEP-B Questionnaires. ILEP Secretariat, London. Single Lesion Multi-Centre Trial Group (1997) Efficacy of single-
ILEP (1999) Guidelines for the Social and Economic Rehabilitation lesion multidrug therapy for the treatment of single-lesion
of People Affected by Leprosy. Second draft. ILEP Secretariat, paucibacillary leprosy. Indian Journal of Leprosy 69, 121129.
London. Smith WCS (1992) The epidemiology of disability in leprosy
Jesudasan K, Vijayakumaran P, Manimizhi N, Jeyarajan T & Rao including risk factors. Leprosy Review 63, S23S3s.
PSS (1996a) Absence of relapse within 4 years among 34 Smith WCS (1997) We need to know what is happening to the
multibacillary patients with high BIs treated for 2 years with incidence of Leprosy. (Editorial). Leprosy Review 68, 195200.
MDT. International Journal of Leprosy 64, 133135. Tulloch J (1999) Integrated approach to child health in developing
Jesudasan K, Vijayakumaran O, Manimozhi N, Rao PSS & Samuel P countries. Lancet 354 (Suppl. II): S16S20.
(1996b) Effectiveness of MDT in multibacillary leprosy. Vadher A & Lalljee M (1992) Patient treatment compliance in
International Journal of Leprosy 64, 128132. leprosy; a critical review. International Journal of Leprosy 60,
Jopling WH (1991) Leprosy stigma. Leprosy Review 62, 112. 587607.
Kawamua HJ, Bwire R & Adatu-Enwgau (1994) Leprosy and Van Beers SM (1998) Leprosy; epidemiological studies of infection
infection with the human immunodeficiency virus in Uganda: a and disease. PhD Thesis, University of Amsterdam.
case-control study. International Journal of Leprosy 62, 521526. Van Beers SM, De Wit MYL & Klatser PR (1996) MiniReview: The
Lambrechts T, Bryce J & Orinda V (1999) Integrated management of epidemiology of Mycobacterium leprae: Recent insight. FEMS
childhood illness: a summary of first experiences. Bulletin of the Microbiology Letters 136, 221230.
World Health Organization 77, 582593. Van Beers SM, Hatta M & Klatser PR (1999a) Patient contact is the
Li HY, Hu LF, Huang WB et al. (1997) Risk of relapse in leprosy major determinant in incident leprosy: implications for future
after fixed duration multidrug therapy. International Journal of control. International Journal of Leprosy 67, 119128.
Leprosy 65, 238245. Van Beers SM, Hatta M & Klatser PR (1999b) Sero-prevalence of
Lietman T, Porco T & Blower S (1997) Leprosy and Tuberculosis: antibodies to phenolic glycolipid-I among children as indicator of
The Epidemiological Consequences of Cross-Immunity. American leprosy endemicity 1999. International Journal of Leprosy 67,
Journal of Public Health 87, 19231927. 243249.
Lockwood DN (1997) Rifampicin/Minocycline and Ofloxacin Van Brakel WH (1999) Proposal regarding MB MDT. (Letter).
(ROM) for single lesions What is the evidence? Leprosy Review Leprosy Review 70, 7173.
68, 299300. Van Brakel WH & Anderson AM (1997) Impairment and disability
Lynch P (1999) Multidrug therapy (Letter). Leprosy Review 70, in leprosy: in search of the missing link. Indian Journal of Leprosy
7071. 69, 361376.
Meima A, Gupte MD, Van Oortmarssen GJ, Habbema JD & Dik J Van Brakel WH, Kist P, Noble S & OToole L (1989) Relapses after
(1997) Trends in Leprosy Case Detection Rates. International multidrug therapy for leprosy: a preliminary report of 22 cases in
Journal of Leprosy 65, 305319. West Nepal. Leprosy Review 60, 4550.
Ministry of Health & Nepal Department of Health Services (1998) Van den Broek J, Chum H, Swai R & OBrien R (1997) Association
Annual Report 1996/1997. MoH, Kathmandu. between leprosy and HIV infection in Tanzania. International
Ministry of Health & Nepal Leprosy Control Division (1999) Final Journal of Leprosy 65, 203210.
Report of Nationwide Leprosy Elimination Campaigns in Nepal. Waters MFR (1998) Is it safe to shorten multidrug therapy for
MoH, Kathmandu. lepromatous (LL and BL) leprosy to 12 months? Leprosy Review
Murray CJL & Lopez AD (1994) Quantifying disability: data, 69, 110111.
methods and results. Bulletin of World Health Organization 72, World Health Organization (1980) International Classification of
481494. Impairments, Disabilities and Handicaps. WHO, Geneva.
Myint T, Thet AT, Htoon MT & Win M (1992) A comparative KAP World Health Organization (1991) World Health Assembly
study of leprosy patients and members of the community in Resolution WHA44.9. WHO, Geneva.
Hlaing and Laung-Lon Townships. Indian Journal of Leprosy 64, World Health Organization (1995) Leprosy disabilities: Magnitude
313324. of the problem. Weekly Epidemiological Record 70, 269276.
Pnnighaus JM & Boerrigter G (1995) Are 18 doses of WHO/MDT World Health Organization (1996) Action Programme for the
sufficient for multibacillary leprosy? Results of a trial in Malawi. Elimination of Leprosy Status Report 1996. WHO/LEP/96.5,
International Journal of Leprosy 65, 17. Geneva.
Pnnighaus JM, Mwanjasi LJ, Fine PEM et al. (1991) Is HIV World Health Organization (1997a) Shortening duration of
infection a risk factor for leprosy? International Journal for treatment of multibacillary leprosy. Weekly Epidemiological
Leprosy 59, 221228. Record 72, 125128.
Raju MS & Kopparty SNM (1995) Impact of knowledge on the World Health Organization (1997b) Progress towards leprosy
attitude towards leprosy patients: a community study. Indian elimination. Weekly Epidemiological Record 72, 165172.
398 2000 Blackwell Science Ltd
Tropical Medicine and International Health volume 5 no 6 pp 388399 june 2000
J. Visschedijk et al. Mycobacterium leprae millennium resistant!
World Health Organization (1998a) WHO Expert Committee on World Health Organization (1998d) Trends in leprosy detection.
Leprosy. Seventh Report. WHO technical Report Series 874. Weekly Epidemiological Record 73, 169176.
WHO, Geneva. World Health Organizaton (1998e) Elimination of leprosy as a
World Health Organization (1998b) Progress towards leprosy public health problem (update). Weekly Epidemiological Record
elimination. Weekly Epidemiological Record 73, 153160. 73, 308312.
World Health Organization (1998c) Leprosy elimination campaigns World Health Organization (1999) Global leprosy situation,
(LECs). Weekly Epidemiological Record 73, 177182. September 1999. Weekly Epidemiological Record 74, 313316.
2000 Blackwell Science Ltd 399
Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Health Law BibliographyDokument11 SeitenHealth Law BibliographyIeien MuthmainnahNoch keine Bewertungen
- Handout CompilationDokument199 SeitenHandout CompilationG Fab100% (2)
- LeprosyDokument32 SeitenLeprosySiselle FajardoNoch keine Bewertungen
- Communicable Disease AnswersDokument11 SeitenCommunicable Disease AnswersRika MaeNoch keine Bewertungen
- Lepra ReactionsDokument16 SeitenLepra ReactionsBimo Aryo TejoNoch keine Bewertungen
- Chelsea's May CurriculumDokument1 SeiteChelsea's May CurriculumIeien MuthmainnahNoch keine Bewertungen
- PPHDokument4 SeitenPPHGwEn LimNoch keine Bewertungen
- CXS 072eDokument17 SeitenCXS 072eIeien MuthmainnahNoch keine Bewertungen
- Uterine Baloon Tamponade FINALDokument11 SeitenUterine Baloon Tamponade FINALIeien MuthmainnahNoch keine Bewertungen
- Uterine AtonyDokument33 SeitenUterine AtonyNonie 'Erni' HastiriniNoch keine Bewertungen
- SOGC Perdarahan Post PartumDokument14 SeitenSOGC Perdarahan Post Partumhi-lineNoch keine Bewertungen
- PPH 2nd Edn Chap-47Dokument6 SeitenPPH 2nd Edn Chap-47Ieien MuthmainnahNoch keine Bewertungen
- Jurnal Microsatelit 3Dokument7 SeitenJurnal Microsatelit 3Ieien MuthmainnahNoch keine Bewertungen
- Jurnal Microsatelit 4Dokument5 SeitenJurnal Microsatelit 4Ieien MuthmainnahNoch keine Bewertungen
- Out Weaned PigDokument9 SeitenOut Weaned PigIeien MuthmainnahNoch keine Bewertungen
- 193 199 1 PBDokument6 Seiten193 199 1 PBAnonymous z0QfbwY3d8Noch keine Bewertungen
- Daftar PustakaDokument1 SeiteDaftar PustakaIeien MuthmainnahNoch keine Bewertungen
- Jurnal Microsatelie 2Dokument7 SeitenJurnal Microsatelie 2Ieien MuthmainnahNoch keine Bewertungen
- Sel DatiaDokument17 SeitenSel DatiaIeien MuthmainnahNoch keine Bewertungen
- Genitmed00058 0033Dokument6 SeitenGenitmed00058 0033Ieien MuthmainnahNoch keine Bewertungen
- Genitmed00058 0033Dokument6 SeitenGenitmed00058 0033Ieien MuthmainnahNoch keine Bewertungen
- Managing Ovarian Masses During Pregnancy - Gary LeiserowitzDokument8 SeitenManaging Ovarian Masses During Pregnancy - Gary Leiserowitzece142Noch keine Bewertungen
- Abdominal Pain During PregnancyDokument58 SeitenAbdominal Pain During Pregnancyquester1515Noch keine Bewertungen
- Viral Diagnostic Tests: 1. HepatitisDokument4 SeitenViral Diagnostic Tests: 1. HepatitisIeien MuthmainnahNoch keine Bewertungen
- Flaps Selected ReadingsDokument78 SeitenFlaps Selected ReadingsIeien MuthmainnahNoch keine Bewertungen
- Malaria Staining BenchaidDokument2 SeitenMalaria Staining BenchaidIeien MuthmainnahNoch keine Bewertungen
- Practitioner Guide To Tzanck Smear Specimen Collection: Limitations and NotesDokument2 SeitenPractitioner Guide To Tzanck Smear Specimen Collection: Limitations and NotesIeien MuthmainnahNoch keine Bewertungen
- Practical Flap Plastic SurgeryDokument10 SeitenPractical Flap Plastic SurgeryPrananingrum Dwi OktarinaNoch keine Bewertungen
- Skin GraftsDokument36 SeitenSkin Graftscado_arifNoch keine Bewertungen
- MMVR09 Local FlapsDokument6 SeitenMMVR09 Local FlapsIeien MuthmainnahNoch keine Bewertungen
- Flaps Selected ReadingsDokument78 SeitenFlaps Selected ReadingsIeien MuthmainnahNoch keine Bewertungen
- Management of Skin LossDokument61 SeitenManagement of Skin LossIeien MuthmainnahNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaIeien MuthmainnahNoch keine Bewertungen
- Clinical Microbiology Reviews-2018-Forbes-e00038-17.fullDokument66 SeitenClinical Microbiology Reviews-2018-Forbes-e00038-17.fullSharwan KumawatNoch keine Bewertungen
- Disease, Death and Control: Missionary Medicine in Colonial ODISHA (1900-1940)Dokument12 SeitenDisease, Death and Control: Missionary Medicine in Colonial ODISHA (1900-1940)TJPRC PublicationsNoch keine Bewertungen
- DR, DR Luh Made Mas Rusyati SPKK (K) Finsdv Dermatology and Venereology Department Medical Faculty Udayana University/ Sanglah HospitalDokument41 SeitenDR, DR Luh Made Mas Rusyati SPKK (K) Finsdv Dermatology and Venereology Department Medical Faculty Udayana University/ Sanglah HospitalJohan CahyadirgaNoch keine Bewertungen
- 4.22 - Quiz LeprosyDokument32 Seiten4.22 - Quiz LeprosyEdo LiawandiNoch keine Bewertungen
- Wonderlic Sample Test (50 Questions)Dokument28 SeitenWonderlic Sample Test (50 Questions)Heather Chavez0% (2)
- Leprosy & Pregnancy: DR Y Sri HarshaDokument53 SeitenLeprosy & Pregnancy: DR Y Sri HarshaBhawna Joshi100% (1)
- SARI Stigma ScaleDokument2 SeitenSARI Stigma ScalerohitNoch keine Bewertungen
- Disorders of HypopigmentationDokument28 SeitenDisorders of HypopigmentationdarkkryNoch keine Bewertungen
- Lab Diagnosis of Leprosy: Moderator: Dr. Bhawesh Koirala Resource: Mr. Tejendra Pandit Speaker: MSMDokument27 SeitenLab Diagnosis of Leprosy: Moderator: Dr. Bhawesh Koirala Resource: Mr. Tejendra Pandit Speaker: MSMMadhusudan MadhavNoch keine Bewertungen
- Leprosy MsDokument78 SeitenLeprosy MsAmit Kochhar67% (3)
- CHN Ii ... Aparna Roll No. 12Dokument17 SeitenCHN Ii ... Aparna Roll No. 12Aparna PandeyNoch keine Bewertungen
- Manual of TB and Leprosy in TanzaniaDokument132 SeitenManual of TB and Leprosy in TanzaniaYovanRivanzahNoch keine Bewertungen
- Topicwise Question RGUHSDokument51 SeitenTopicwise Question RGUHSKohenNoch keine Bewertungen
- Disease Research PaperDokument6 SeitenDisease Research PaperJose PalaciosNoch keine Bewertungen
- Disabilties and Deformities in Leprosy Seminar14!4!2017Dokument21 SeitenDisabilties and Deformities in Leprosy Seminar14!4!2017Rohit GuptaNoch keine Bewertungen
- Bacillary DysenteryDokument8 SeitenBacillary DysenteryRijane Tabonoc OmlangNoch keine Bewertungen
- Annual Report 2067 68 Final PDFDokument399 SeitenAnnual Report 2067 68 Final PDFBijay Poudel100% (1)
- Leprosy QiuzDokument65 SeitenLeprosy QiuzDurgaMadhab Tripathy100% (1)
- The History of Leprosy in CambodiaDokument64 SeitenThe History of Leprosy in CambodiaNeakreach PichNoch keine Bewertungen
- Community Health NursingDokument40 SeitenCommunity Health NursingBONGNoch keine Bewertungen
- Derma Trans Clerks Review 2019Dokument22 SeitenDerma Trans Clerks Review 2019anonymousNoch keine Bewertungen
- Case Definition Infectious Disease 2016Dokument143 SeitenCase Definition Infectious Disease 2016unit cdc pkd raubNoch keine Bewertungen
- The Origin and Spread of Leprosy: Historical, Skeletal, and Molecular DataDokument30 SeitenThe Origin and Spread of Leprosy: Historical, Skeletal, and Molecular DataNaeNoch keine Bewertungen
- Dols (Michael W.) - The Leper in Medieval Islamic Society (Speculum 58:4, 1983, 891-916)Dokument27 SeitenDols (Michael W.) - The Leper in Medieval Islamic Society (Speculum 58:4, 1983, 891-916)juanpedromolNoch keine Bewertungen
- Case 4. Leprosy and Reaction For Tutor Guide-Revisi 161120Dokument25 SeitenCase 4. Leprosy and Reaction For Tutor Guide-Revisi 161120Raihan IsvandiarNoch keine Bewertungen
- References Stigma and EpidemicsDokument280 SeitenReferences Stigma and EpidemicsadripfNoch keine Bewertungen