Das könnte Ihnen auch gefallen
- Aktivasi Win10proDokument1 SeiteAktivasi Win10provinoadhiyogaNoch keine Bewertungen
- Anti CCP American College of Rheumatology CriteriaDokument2 SeitenAnti CCP American College of Rheumatology CriteriahprafullNoch keine Bewertungen
- Management of Hyperglycemia and Diabetes in The HospitalDokument46 SeitenManagement of Hyperglycemia and Diabetes in The HospitalvinoadhiyogaNoch keine Bewertungen
- Buku Saku Event 2020 Harmony (Final 00)Dokument78 SeitenBuku Saku Event 2020 Harmony (Final 00)Abdullah Shidqul Azmi100% (10)
- ESA Statement SJS HLADokument3 SeitenESA Statement SJS HLAvinoadhiyogaNoch keine Bewertungen
- Antigen Dalam Tiroid AutoimunDokument29 SeitenAntigen Dalam Tiroid AutoimunvinoadhiyogaNoch keine Bewertungen
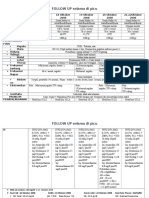
- Follow Up Selama Di PICUDokument2 SeitenFollow Up Selama Di PICUvinoadhiyogaNoch keine Bewertungen
- Buku Saku Event 2020 Harmony (Final 00)Dokument78 SeitenBuku Saku Event 2020 Harmony (Final 00)Abdullah Shidqul Azmi100% (10)
- Follow Up Selama Di PICUDokument2 SeitenFollow Up Selama Di PICUvinoadhiyogaNoch keine Bewertungen
- Read MeDokument49 SeitenRead MePriyawan SukisnoNoch keine Bewertungen
- Antigen Dalam Tiroid AutoimunDokument5 SeitenAntigen Dalam Tiroid AutoimunvinoadhiyogaNoch keine Bewertungen
- Portofolio Kasus Bedah CoverDokument1 SeitePortofolio Kasus Bedah CovervinoadhiyogaNoch keine Bewertungen
- Gangguan WahamDokument11 SeitenGangguan WahamvinoadhiyogaNoch keine Bewertungen
- Gambar Bedah UrangDokument4 SeitenGambar Bedah UrangvinoadhiyogaNoch keine Bewertungen
- Portofolio Kasus Bedah CoverDokument1 SeitePortofolio Kasus Bedah CovervinoadhiyogaNoch keine Bewertungen
- Granulating Tissue 1-2 Weeks GraftingDokument8 SeitenGranulating Tissue 1-2 Weeks GraftingvinoadhiyogaNoch keine Bewertungen
- Portofolio Kasus Medis Abses Hepar CoverDokument1 SeitePortofolio Kasus Medis Abses Hepar CovervinoadhiyogaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Infection ControlDokument58 SeitenInfection ControlYoyen Gonzaga100% (10)
- 1 Objectives and Classification PD FayadDokument25 Seiten1 Objectives and Classification PD FayadMostafa FayadNoch keine Bewertungen
- Clinical Diagnostic Criteria For AD and FTDDokument2 SeitenClinical Diagnostic Criteria For AD and FTDdogstar23Noch keine Bewertungen
- Mr. Abhishek Sharma-1Dokument3 SeitenMr. Abhishek Sharma-1Abhishek SharmaNoch keine Bewertungen
- Assessment Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation EffectivenessDokument3 SeitenAssessment Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation EffectivenessYnah Sayoc75% (4)
- Discharge advice after coronary proceduresDokument12 SeitenDischarge advice after coronary proceduresEmma EmilyNoch keine Bewertungen
- ConcussionDokument6 SeitenConcussionradziah_mohdNoch keine Bewertungen
- C SectionDokument7 SeitenC SectionJet-Jet GuillerganNoch keine Bewertungen
- Annotated BibliographyDokument3 SeitenAnnotated Bibliographyapi-240834444Noch keine Bewertungen
- ImdrfDokument30 SeitenImdrfborrellanoNoch keine Bewertungen
- Tooth Eruption and Its Disorders - Pediatric DentistryDokument157 SeitenTooth Eruption and Its Disorders - Pediatric DentistryPuneet ChoudharyNoch keine Bewertungen
- Cup of Kindness: NHS Greater Glasgow and ClydeDokument16 SeitenCup of Kindness: NHS Greater Glasgow and ClydecrispypataNoch keine Bewertungen
- Graded Exercise Testing (GXT) NewDokument8 SeitenGraded Exercise Testing (GXT) Newf3rd110Noch keine Bewertungen
- Assessing and Treating Pediatric Anxiety DisordersDokument19 SeitenAssessing and Treating Pediatric Anxiety Disordersayub01Noch keine Bewertungen
- Biopure Case Solution: Havard Business School CaseDokument4 SeitenBiopure Case Solution: Havard Business School Caseparoengineer75% (4)
- Yemisi Chapter ThreeDokument10 SeitenYemisi Chapter ThreeAbimbola OyarinuNoch keine Bewertungen
- 256 CircumcisionDokument5 Seiten256 CircumcisionMD Luthfy LubisNoch keine Bewertungen
- Myocardial Infarct Checklist: TIMELINE // DateDokument2 SeitenMyocardial Infarct Checklist: TIMELINE // DateMohd Syamirulah RahimNoch keine Bewertungen
- Neurogenic Bladder: When Nerve Damage Causes Bladder ProblemsDokument3 SeitenNeurogenic Bladder: When Nerve Damage Causes Bladder ProblemsmarselamgeNoch keine Bewertungen
- Angina PectorisDokument4 SeitenAngina PectorisAnn CunananNoch keine Bewertungen
- Acute Flaccid ParalysisDokument36 SeitenAcute Flaccid ParalysisArun George100% (1)
- Strabismus surgery outcomes without buckle removalDokument5 SeitenStrabismus surgery outcomes without buckle removalBima RizkiNoch keine Bewertungen
- Hospital Indemnity Claim Form: Policy NumberDokument2 SeitenHospital Indemnity Claim Form: Policy NumberMoyo Mitchell0% (1)
- Cardiac Complications in Diphtheria Predict OutcomesDokument12 SeitenCardiac Complications in Diphtheria Predict OutcomesPratiwi Indah PalupiNoch keine Bewertungen
- StreptokinaseDokument3 SeitenStreptokinaseKashif SanwalNoch keine Bewertungen
- Tugas English of NursingDokument3 SeitenTugas English of NursingSyahlu DamayantiiNoch keine Bewertungen
- OB MedsDokument19 SeitenOB Medsohsnapitslei100% (2)
- Sanford Resume 3 21 18Dokument2 SeitenSanford Resume 3 21 18api-329968843Noch keine Bewertungen
- SimuzazuDokument3 SeitenSimuzazuhelenjamelamulengaNoch keine Bewertungen